
SPORTS PODIATRY – SESAMOIDITIS – ALICANTE
Sesamoiditis treatment: return to pain-free running at the base of the big toe
Stepwise protocol with unloading insoles, ultrasound-guided infiltration and MIS sesamoidectomy – Faster return to sport than with open surgery – 45 years treating the athlete’s foot.
Backed by 45 years of experience in forefoot pathology
Clinic founded in 1979
Three generations treating athletes, dancers and patients with forefoot pain in Alicante.
Certification MIS23BE03
Accredited by the American Board of Multispecialty Podiatry for minimally invasive surgery.
Multilingual service
We attend you in Spanish, English, German, French and Dutch.
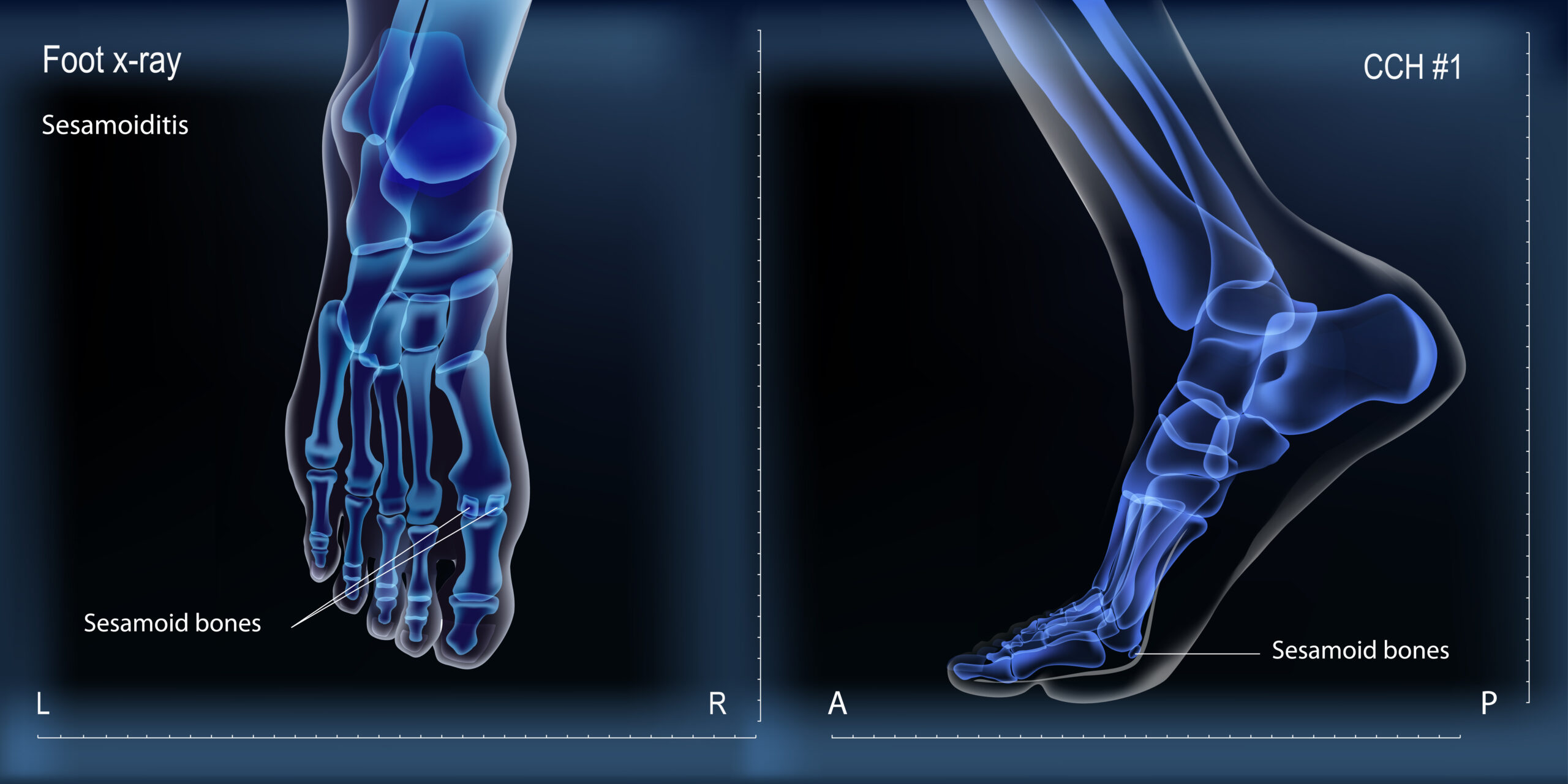
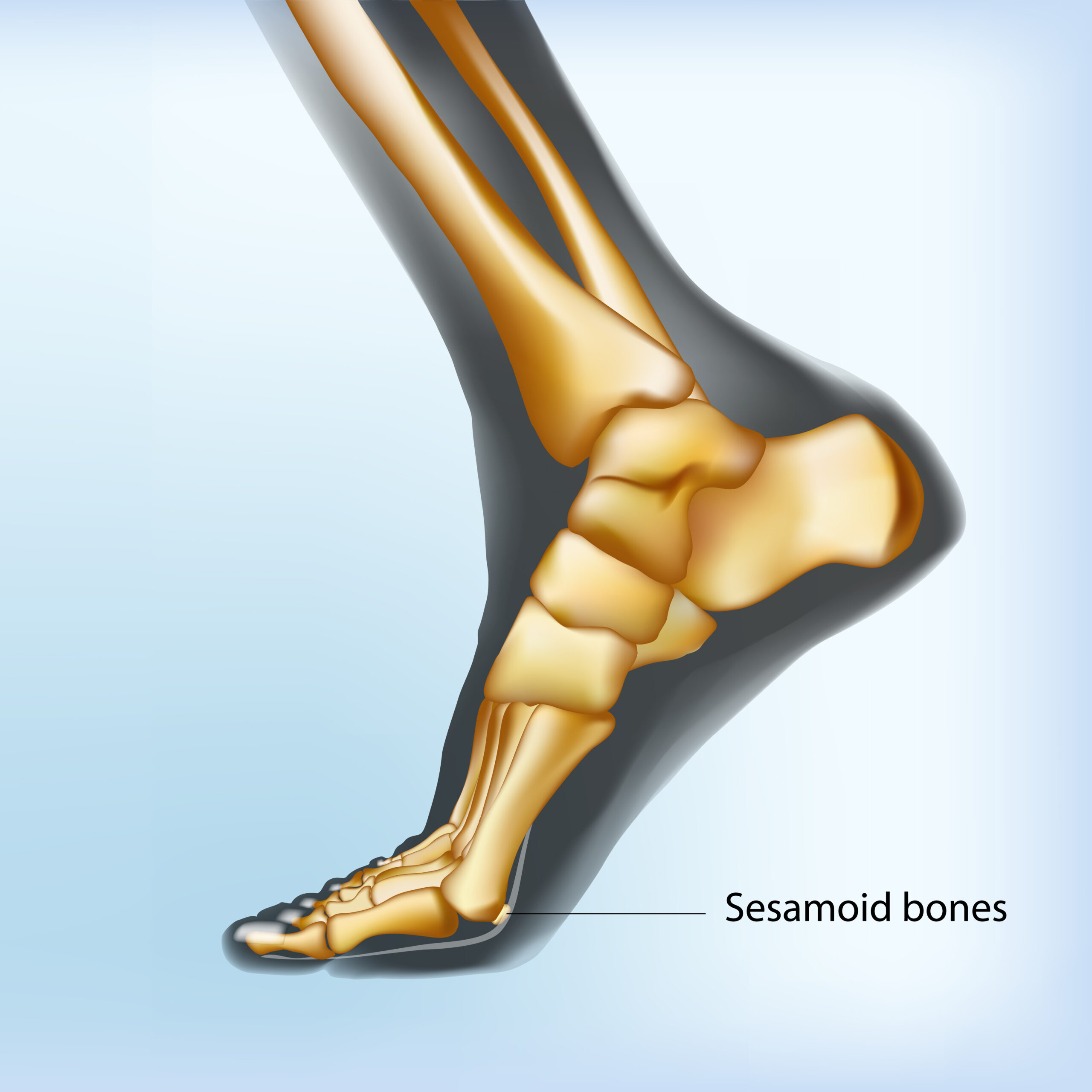
What is sesamoiditis?
Sesamoiditis is inflammation of the sesamoid bones and surrounding tendon structures at the head of the first metatarsal. The sesamoids are two small bones – medial (tibial) and lateral (peroneal) – housed within the tendon of the flexor digitorum brevis muscle, just below the metatarsophalangeal joint of the first toe. They function as true biological pulleys: they cushion the load during stance, improve flexor leverage and absorb up to 50% of body weight in each toe-off phase of walking or running.
When this load becomes excessive or repetitive, the cartilage, the tendon and the bone itself can become inflamed, causing a very characteristic pain in the sole of the foot, just under the big toe. Sesamoiditis is responsible for 5-9% of foot injuries in athletes according to various classic series, with a clear predilection for long-distance runners, ballet dancers, gymnasts, basketball players and women who regularly wear high heels.
At Clínica San Román we approach sesamoiditis with a staggered protocol: we start with custom insoles and activity modification, escalate to ultrasound-guided infiltration when pain persists and, in refractory cases or with fracture/osteonecrosis, we offer minimally invasive sesamoidectomy, which allows a significantly faster return to sports than traditional open surgery.
Symptoms: How to recognize sesamoiditis?
The pain of sesamoiditis is very localized and recognizable: it appears just below the base of the big toe, intensifies on foot strike and worsens with any activity that increases pressure on the forefoot. Most patients describe a progressive history of weeks or months, without a single blow, in which the pain sets in until it limits training, dancing or simply wearing heels.
- Pain in the plantar aspect of the head of the first metatarsal, under the big toe, when resting.
- Pain that increases with dorsal flexion of the first toe (climbing stairs, take-off position when running).
- Worsening with high heels, ballet flats or thin-soled shoes.
- Discrete swelling, erythema and local temperature increase.
- Selective tenderness on palpation of the medial sesamoid (more frequent) or lateral sesamoid.
- Lameness or “supination gait” to avoid loading the first radius.
- Morning stiffness of the first finger in prolonged pictures.
- Occasional crepitus on mobilization of the big toe joint.
Why does sesamoiditis appear?
Sesamoiditis is almost always the result of sustained overload on two tiny bones designed to absorb shock, not to withstand chronic friction. Understanding why they are overloaded is key to treating it well and, above all, to ensuring that it does not recur once it is resolved.
🏃 Sports overload
Repeated toe-off gestures – running, jumping, pointe dancing, braking and starting in racquet sports – multiply the load on the sesamoids. Several studies (Boike, Cohen) place sesamoiditis among the five most frequent causes of metatarsalgia in long-distance runners and classical ballet dancers. Sudden increases in training volume, changes of surface (track to asphalt), very worn shoes and poor technique are the most common precipitating factors.
👠 Unsuitable footwear
High heels shift up to 75% of body weight to the forefoot, overloading the sesamoids. Soles that are too thin (poorly adapted minimalist shoes), shoes that are too stiff in the metatarsophalangeal flexion zone or dance/climbing shoes with sustained plantar compression are frequent aggressors. This is the reason why the condition is so typical in women around 30-45 years of age with prolonged use of heels and in professional dancers.
🦶 Cavus foot or pronated forefoot
Cavus feet support more load on metatarsal heads and, therefore, on sesamoids. The pronated forefoot (varus of the rearfoot with pronator compensation of the forefoot) selectively overloads the medial sesamoid. Hallux valgus, long (Egyptian) big toe, limb dysmetry and first radius stiffness also play a role. Detecting this biomechanical substrate with a gait analysis is decisive to avoid relapses.
Diagnosis: how do we confirm sesamoiditis?
Correctly confirming sesamoiditis and, above all, ruling out fracture, osteonecrosis or turf toe is what separates a quick recovery from months of frustrating evolution. At Clínica San Román we protocolize the diagnosis in three complementary levels:
🔍 Clinical exploration and selective palpation
We locate the pain with digital palpation over the medial and lateral sesamoid. We reproduce the symptoms with the passive dorsal flexion maneuver of the first toe (which tightens the short flexor over the sesamoids) and assess the mobility of the first radius, possible associated deformities (hallux valgus, hallux rigidus) and the static and dynamic tread pattern.
📷 X-ray with axial projection
We request dorsoplantar radiography, lateral in load and, above all, axial projection of the sesamoid, essential to evaluate morphology, rule out fractures, assess diastasis (separation) between the poles of the bipartite sesamoid and observe signs of degeneration. The simple radiography is the first imaging test and, in many cases, it is enough to orient the picture.
🔊 Ultrasound and magnetic resonance imaging
MRI is the gold standard: it can distinguish simple sesamoiditis, stress fracture, sesamoid osteonecrosis (characteristic bone edema) and plantar plate lesions. Dynamic ultrasound is useful to assess adjacent bursitis and guide therapeutic infiltration with millimeter precision. In selected cases, bone scintigraphy provides complementary information.
Treatment of sesamoiditis: stepwise protocol
The philosophy is less is more. The vast majority of sesamoiditis resolves with well-done conservative treatment. Only refractory cases, those with unconsolidated fractures or osteonecrosis reach the operating room. When they do, MIS surgery makes the difference in speed of recovery.
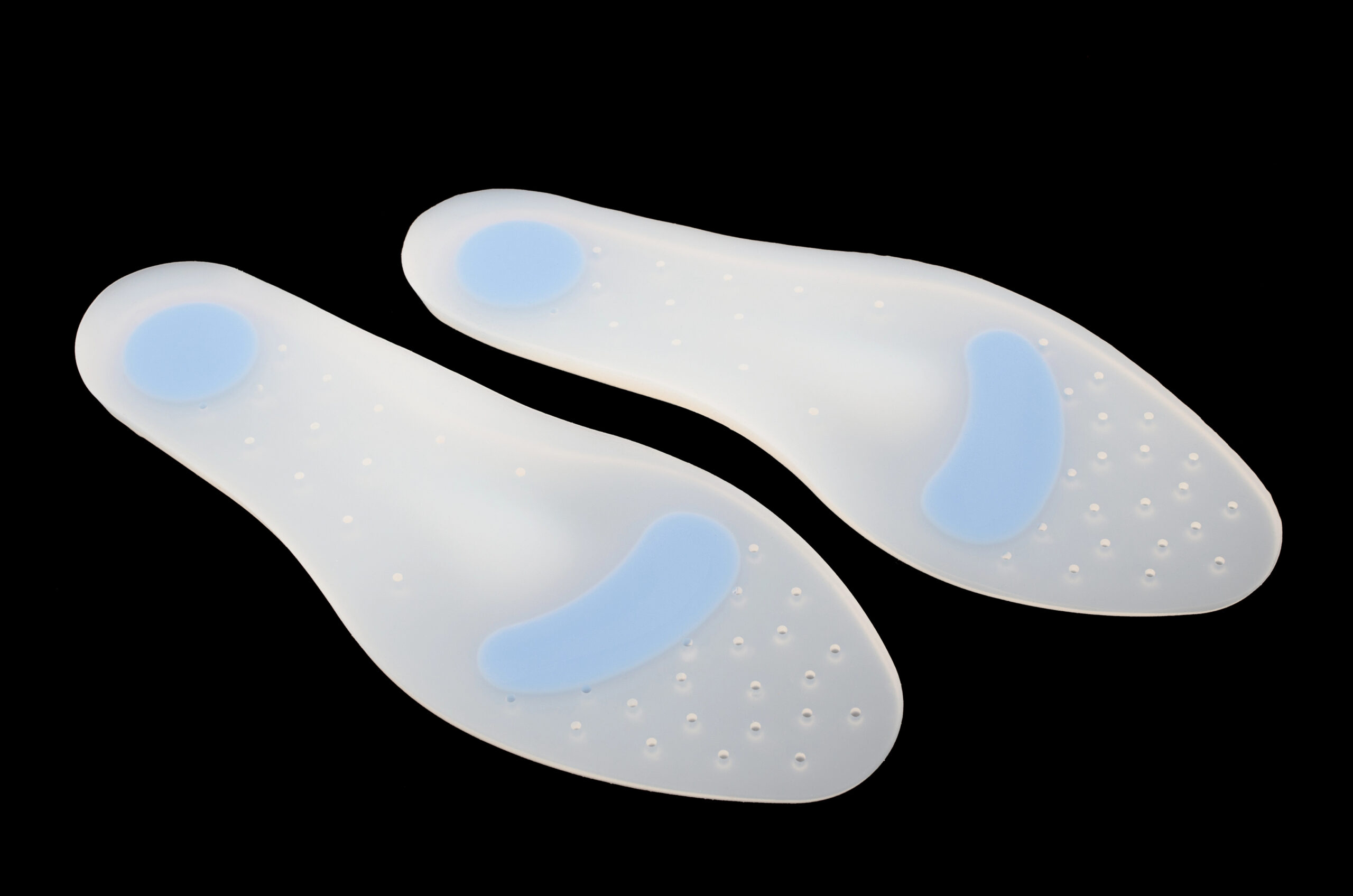
1 Conservative treatment: active rest and unloading
It is the base. It combines relative sports rest (maintain cardiovascular activity without impact: cycling, elliptical, swimming), custom insoles with sesamoid relief (classic “U” or “donut” in thermoplastic/EVA that surrounds the sesamoids without pressing them), modification of footwear (rigid sole in the flexion area, eliminate high heels), NSAIDs by mouth for 7-10 days, local ice and physiotherapy to release the plantar fascia and the flexor tendon. Various series place the response to conservative treatment at around 70-85% of cases at 8-12 weeks (Sims, World J Orthop 2014).
2 Echoguided infiltration
When pain persists after 6-8 weeks of correctly performed conservative treatment, we consider ultrasound-guided infiltration of the peri-sesamoid space. We use prolonged-release corticosteroid or platelet-rich plasma (PRP) depending on the patient’s profile and clinical stage. Ultrasound guidance guarantees millimetric precision and minimizes the risk of intratendinous injection. Combined with insoles and sports rest, it is usually sufficient to resolve the condition or to allow a gradual return to activity.
3 Minimally Invasive Sesamoidectomy (MIS)
Reserved for sesamoiditis refractory to 6 months of well-established treatment, unconsolidated fractures, osteonecrosis confirmed by MRI and cases with persistent symptomatic bipartism. MIS sesamoidectomy consists of percutaneous excision of the affected sesamoid (medial or lateral) by means of a millimetric incision, under local anesthesia and intraoperative radiological control. Compared to open surgery, MIS better preserves the insertions of the short flexor, drastically reduces postoperative pain and shortens the return to sport. The vast majority of patients return to light activity at 4-6 weeks and to impact sports at 10-14 weeks (Cohen, Foot Ankle Clin 2009).
Comparison of sesamoiditis treatments
| Criteria | Template + rest | Ultrasound-guided infiltration | MIS sesamoidectomy | Open surgery |
|---|---|---|---|---|
| Indication | First line, all patients | Persistent pain >6-8 weeks despite conservative treatment | Refractory >6 months, ununited fracture, osteonecrosis | Complex cases, associated deformity, previous MIS failure |
| Invasiveness | Null | Minimal (ultrasound-guided puncture) | 3-4 mm incision, ambulatory | Wide plantar or medial incision |
| Anesthesia | – | Local infiltrative | Local truncal | Local with sedation or regional |
| Time / sessions | 8-12 weeks | 1-3 sessions spaced 4-6 weeks apart | 20-40 min – same day discharge | 30-60 min – outpatient or 24 h admission |
| Efficacy | ≈70-85 % (Sims 2014). | Adjuvant; 50-70 % improvement at 3-6 months. | High (≈85-90 %) with faster sports return. | High, but more residual stiffness and longer downtime. |
Source: Sims AL, Kurup HV. World J Orthop 2014; Boike A et al, Clin Podiatr Med Surg 2011; Cohen BE. Foot Ankle Clin 2009. Individual results may vary.
Advantages of MIS sesamoid surgery
You walk the same day
Immediate discharge with post-surgical forefoot off-loading shoe. No cast, no admission.
Local anesthesia
Truncal block of the first finger. Without general sedation, without prolonged fasting.
Millimeter incision
3-4 mm incision that heals almost imperceptibly. Aesthetic result far superior to open surgery.
Rapid sporting return
Light activity 4-6 weeks, impact sport 10-14 weeks. Significantly less than open surgery.
Preserves biomechanics
Respect flexor digitorum brevis insertions and plantar plate as much as possible. Less residual stiffness of the first toe.
High documented efficiency
Resolution of pain in about 85-90% of cases in specialized literature (Cohen, 2009).
Prevention of sesamoiditis
Sesamoiditis recurs relatively frequently if the factors that triggered it are not corrected. These three levers summarize what we ask of our patients once the acute episode is resolved:
👟 Suitable footwear
Sole with good shock absorption in the forefoot area, removable insole (to use the customized one), moderate heel in daily use and sports shoe renewed every 600-800 km of running. Limit high heels to occasional occasions and avoid shoes with soles that are too thin or completely flat for prolonged activity.
🦵 Exercises and proprioception
Isometric work of the short flexor of the first toe, stretching of the plantar fascia and triceps suralis, proprioception exercises on unstable surfaces and strengthening of the intrinsic musculature of the foot. A correct sports progression (weekly load increases of less than 10%) significantly reduces the risk of relapse.
⚖️ Templates and weight
In patients with predisposing biomechanical factors (cavus foot, pronated forefoot, hallux valgus), custom insoles are a preventive investment. Controlling body weight, especially during impact activity, also directly unloads the sesamoid region. Annual podiatric checkup if you have a history of or practice high-impact sports.

Have you been experiencing pain in the base of your big toe when running or walking for months?
Sesamoiditis is effectively treated and rarely requires surgery. We study your footprint, rule out fracture or osteonecrosis and design a plan that returns you to sport without pain.
Request your free evaluationFrequently asked questions about sesamoiditis
We solve the most common doubts of our patients.
🔬 About the pathology.
Is it the same as a bunion?
No. The bunion (hallux valgus) is a lateral deviation of the big toe with medial bony prominence in the head of the first metatarsal. Sesamoiditis is an inflammation of the sesamoid bones located under that same metatarsal. They can coexist – in fact, hallux valgus is a risk factor for sesamoiditis – but the pain is different: the bunion hurts laterally, sesamoiditis hurts on the sole. Confirming the difference is key because treatment varies substantially.
Sesamoiditis or sesamoid fracture: how do they differ?
Clinically, it is difficult to differentiate between them: both hurt when resting and worsen with dorsal flexion. The difference is in the image. Sesamoiditis shows bone edema in MRI without fracture line. Acute fracture shows radiolucent line with irregular borders; stress fracture appears as intense bone edema with or without visible fracture line. A detail: the bipartite sesamoid (anatomical variant with smooth and symmetrical borders) is often mistaken for a fracture. That is why radiography and, when in doubt, MRI are essential.
Why does it take so long to heal?
Sesamoids are small bones, without direct contact with continuous bone tissue and with scarce terminal vascularization. When inflamed or fractured, the limited blood supply delays healing. In addition to the fact that each step places a significant load on the area, healing or resolution of the inflammation requires weeks or even months of actual, not relative, unloading. A small percentage of fractures progress to nonunion and an even smaller percentage to osteonecrosis (Renander’s disease).
Can I continue training with sesamoiditis?
In the acute phase, impact sports are contraindicated: each step reactivates inflammation and prolongs the injury. You can maintain cardiovascular work without impact: cycling, elliptical, swimming with equipment or with the first toe well protected and strength training without painful support. The return to running or dancing is planned to be progressive, once the pain disappears in walking and in selective load tests. Forcing earlier usually means repeating the cycle from the beginning.
🏥 Treatment
Do the templates work in all cases?
Sesamoid offloading inserts are the first line of treatment and resolve a considerable majority of cases on their own or in combination with rest and NSAIDs. Several studies put the response at 70-85% at 8-12 weeks (Sims, 2014). Their success depends on three factors: that they are well designed (real unloading of the affected sesamoid, not generic), that they are accompanied by appropriate footwear and that the patient respects sports rest during the acute phase. They are not a universal solution: if they fail, we escalate to infiltration or surgery.
Are infiltrations safe?
Performed under ultrasound guidance and by experienced professionals, peri-sesamoid infiltrations are safe and painless. We use extended-release corticosteroid or platelet-rich plasma (PRP) depending on the case. We limit the number (rarely more than 2-3 sessions) to avoid tissue atrophy or risk of tendon rupture, and we always combine them with insoles and biomechanical work so that the improvement is sustained and not a temporary patch.
Does operating the sesamoid affect foot support?
Sesamoidectomy is planned to minimize biomechanical impact. Removing only one sesamoid (medial or lateral, the affected one) is well tolerated in most patients, although a small loss of toe-off strength of the first toe and, in some cases, progressive hallux varus or valgus deformity may occur if the insertions are not respected. We never remove both sesamoids at the same time unless there is a major cause: doing so is associated with significant weakness of the first radius and secondary deformities. The MIS technique preserves the neighboring structures better than open surgery.
🏃 Recovery and prevention
How long does sports recovery take?
After conservative treatment, return to running or dancing usually occurs between 8 and 12 weeks with insoles and progressive work. After infiltration, relief appears at 7-14 days and return to full sport at 4-6 weeks. After MIS sesamoidectomy, we schedule light activity (cycling, swimming) from the 4th-6th week and impact sports between the 10th and 14th week, always with clinical and radiological assessment. Traditional open surgery tends to extend these periods by several weeks.
Can it recur?
Yes, especially if the predisposing factors are not corrected: foot biomechanics, footwear, sports technique and training load. Sesamoiditis treated only with NSAIDs or rest, without addressing the cause, often recurs when returning to sport. That is why our protocol always includes gait analysis, personalized maintenance insole, footwear review and sports progression guideline. After a well-indicated sesamoidectomy, recurrence of the original condition is rare, although pain may appear in the opposite sesamoid if the biomechanics are still altered.
Can I prevent it if I am a runner or dancer?
To a large extent, yes. The keys: gradual progression of loads (no more than 10% per week), proper shoes and renewed on time, foot strength work, proprioception, weight control and, if you have a cavus foot or pronated forefoot, custom insoles as a preventive measure. In dancers, the technique of rising to pointe and the dosage of classes are decisive. An annual sports podiatry check-up is the most effective way to detect risk factors before they turn into injury.
Scientific references
- Sims AL, Kurup HV. Painful sesamoid of the great toe. World J Orthop. 2014;5(2):146-50. [PMID: 24829878]
- Boike A, Schnirring-Judge M, McMillin S. Sesamoid disorders of the first metatarsophalangeal joint. Clin Podiatr Med Surg. 2011;28(2):269-85. [PMID: 21669340]
- Cohen BE. Hallux sesamoid disorders. Foot Ankle Clin. 2009;14(1):91-104. [PMID: 19232994]
- Dedmond BT, Cory JW, McBryde A Jr. The hallucal sesamoid complex. J Am Acad Orthop Surg. 2006;14(13):745-53. [PMID: 17148622]
- Richardson EG. Injuries to the hallucal sesamoids in the athlete. Foot Ankle. 1987;7(4):229-44. [PMID: 3817664]
- Bichara DA, Henn RF 3rd, Theodore GH. Sesamoidectomy for hallux sesamoid disorders. Foot Ankle Int. 2012;33(9):704-6. [PMID: 22995256]
Information prepared by the medical team of Clínica San Román. Center No. 5357 Autonomous Registry of Health Centers, Services and Establishments of the Valencian Community. This page is for information purposes only and does not replace the individual clinical assessment.
Don’t let the pain of sesamoiditis control your sport
We study your footprint, rule out fracture or osteonecrosis and design a step-by-step plan to get you back to training without pain. We have been doing it for 45 years in Alicante.
- 📞 +34 965 921 156
- ✉️ info@clinicasanroman.com
- Av. del Dr. Ramón y Cajal 1, 03001 Alicante