
PODIATRY – BIOMECHANICS – SURGERY MY – ALICANTE
Cavus foot treatment: stabilizes the ankle, unloads the forefoot and restores pain free walking
Structured diagnosis of flexible and rigid cavus foot. Shock absorbing insoles, forefoot MIS surgery and neurological coordination when appropriate. 45 years specializing in foot biomechanics.

45 years specializing in foot pathology
Clinic founded in 1979
Three generations treating pediatric, adult and athletic cavus feet.
Certification MIS23BE03
Accredited by the American Board of Multispecialty Podiatry for minimally invasive surgery.
Multilingual service
We attend you in Spanish, English, German, French and Dutch.
What is cavus foot?
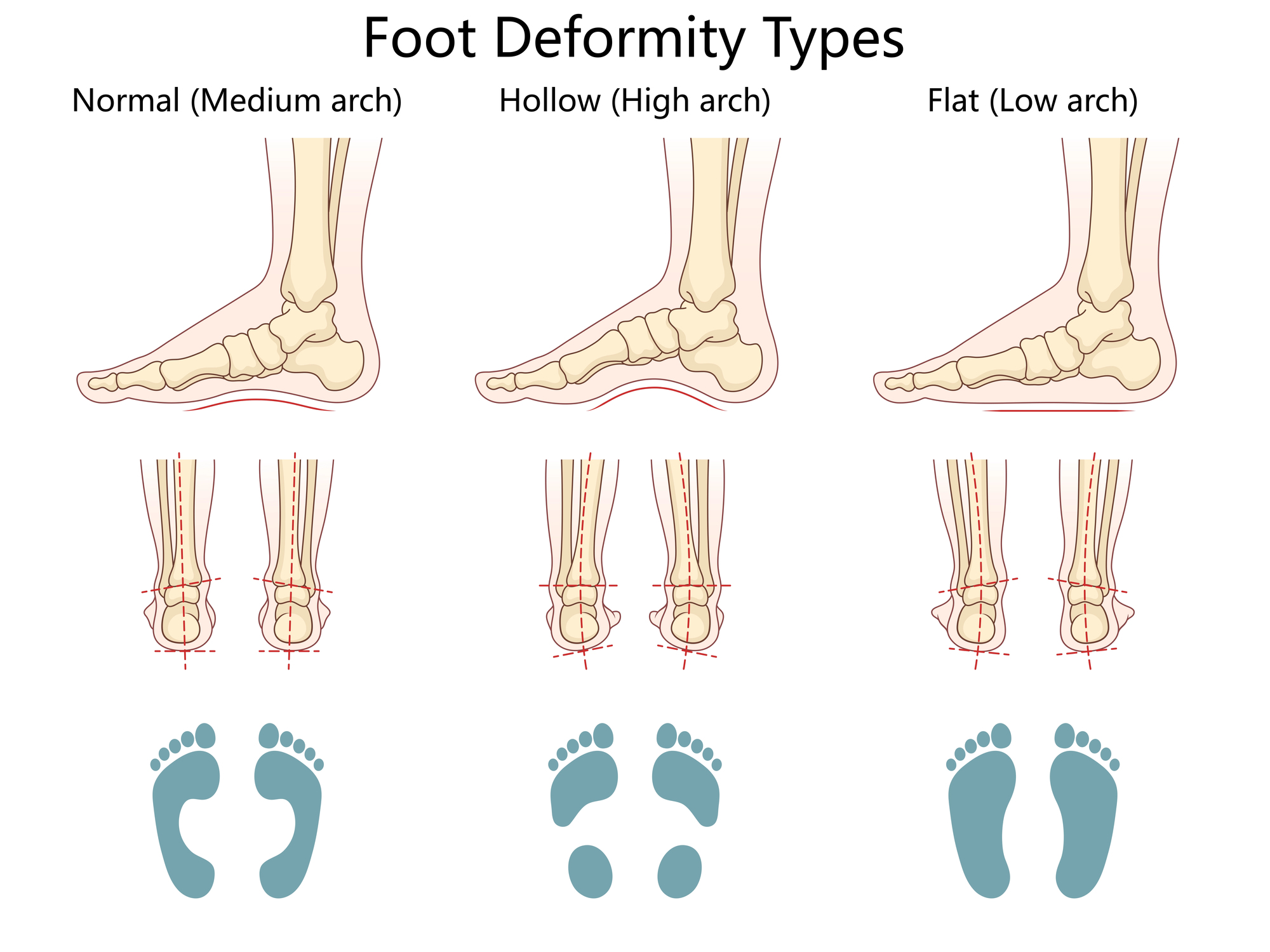
The cavus foot (pes cavus) is the opposite structural deformity to the flatfoot: the internal longitudinal arch is exaggeratedly elevated, the rearfoot is usually in varus (heel tilted outward) and the forefoot in fixed plantar flexion (forefoot equinus). The result is a stiff foot, with poor shock absorption capacity, bearing load predominantly on the heel and metatarsal heads and leaving the midfoot almost without contact with the ground.
This abnormal load distribution generates a recognizable clinical pattern: metatarsalgia, claw toes, calluses on metatarsal heads and base of the 5th toe, recurrent ankle sprains due to lateral instability, atypical plantar fasciitis and peroneal tendinopathy due to overloading of the outer edge. In a relevant proportion of cases -especially when bilateral, symmetrical and progressive- cavus foot is the first manifestation of an underlying hereditary neuropathy, typically Charcot-Marie-Tooth disease.
At Clínica San Román we approach cavus foot as a biomechanical deformity with an etiology that should be ruled out. We combine structured diagnosis, specific shock absorbing insoles, minimally invasive surgery of the forefoot when appropriate and coordination with neurology in cases of neuromuscular suspicion.
Symptoms: how does a symptomatic cavus foot manifest itself?
An asymptomatic cavus foot in a patient without progression or associated pathology may not require treatment. But the majority of cavus feet in consultation are accompanied by a procession of symptoms that limit quality of life and justify a structured assessment.
- Metatarsalgia: mechanical pain in metatarsal heads with walking or sports, with visible calluses.
- Claw toes or hammer toes, especially 2nd to 5th toes, with dorsal chafing in footwear.
- Stiff and poorly cushioned foot sensation, rapid fatigue during sustained walking.
- Pain in the lateral aspect of the foot and ankle due to overload of the 5th metatarsal and peroneals.
- Recurrent ankle sprains, sensation of lateral instability.
- Characteristic plantar calluses on metatarsal heads and base of the 5th toe.
- Atypical plantar fasciitis, external heel pain.
- Difficulty finding comfortable shoes (high instep, narrow forefoot).
- In neurological cases: foot drop, clumsiness in running, frequent falls, selective muscle fatigue.
Why does cavus foot appear?
Unlike flatfoot, cavus foot is almost never the result of simple overload: in most cases there is an underlying muscular imbalance, congenital or acquired, that pulls the foot towards this morphology.
🧬 Hereditary neuropathies
Charcot-Marie-Tooth disease is the most common neurological cause of cavus foot. It is a hereditary neuropathy, genetically determined, which causes selective weakness of peroneal and intrinsic musculature of the foot, leaving the flexors and supinators not counterbalanced to progressively deform the foot. Other hereditary neuropathies and ataxias (Friedreich) produce similar pictures. Therefore, when faced with progressive bilateral cavus foot, especially in children/adolescents, neurological assessment is always advisable.
🧠 Acquired neurological causes.
Sequelae of poliomyelitis, cerebral palsy, spina bifida, spinal cord injuries, stroke with selective involvement of distal musculature, traumatic neuropathies of the common peroneal and, in rare cases, conus medullaris tumors. The detection of these causes modifies the prognosis and the therapeutic plan: sometimes the podiatrist is the first professional to detect the problem and refer.
🦶 Idiopathic and biomechanical
A percentage of cavus feet have no identifiable cause: they are idiopathic, usually stable, non-progressive and manageable with conservative treatment. There are also cavus feet due to chronic contracture of the triceps suralis (equinus), sequelae of poorly consolidated fractures or previous surgeries. The so-called “subtle cavus foot” (Manoli, 2005) describes mild forms that are frequently underdiagnosed and are responsible for chronic ankle sprains and stress fractures of the 5th metatarsal in athletes.
Diagnosis: how do we evaluate cavus foot?
Diagnosis of cavus foot goes beyond measuring arch height. It is necessary to differentiate flexible/rigid, identify the etiology when it exists, map the associated pathologies (claw toes, lateral instability, metatarsalgia) and plan the order of treatment. At Clínica San Román we structure the assessment in four levels.
🔍 Structured exploration
We observe the patient in standing, walking and on tiptoe. We apply the Coleman test (block test): if when the block is placed only on the lateral edge of the foot the heel is corrected, the cavus foot is of anterior and flexible origin; if it is not corrected, there is a rigid component of the rearfoot. We also evaluate foot drop, peroneal strength, claw toes, plantar calluses and family history of cavus feet.
📊 Biomechanical pressure study
Prescan footprint analysis: objectively documents the loading pattern in the heel, metatarsal heads and lateral border, the lack of midfoot support and the asymmetries between both feet. It is essential information for designing shock-absorbing insoles with effective selective offloading and for documenting improvement after treatment.
📷 Bilateral loading radiography
Dorsoplantar, lateral loading and axial projection of the calcaneus. Measures the Meary-Tomeno angle (talus-1st metatarsal axis), Hibbs angle (calcaneus-1st metatarsal axis), calcaneal tilt angle and signs of associated joint subluxation. It documents the magnitude of the deformity and guides the type of surgery if indicated.
🧠 Complementary neurological assessment.
In patients with bilateral, symmetrical, progressive cavus feet or with a family history, we request electromyography and referral to neurology to rule out Charcot-Marie-Tooth and other neuropathies. Lumbar spine MRI is indicated in unilateral or atypical cavus feet to rule out spinal cord pathology. The etiology changes the follow-up.
Treatment of cavus foot: stepwise protocol
As in the rest of biomechanical pathologies, the principle is the minimum necessary treatment. Most symptomatic cavus feet are controlled with conservative treatment. Surgery is reserved for refractory or progressive cases and is always planned from less to more invasive.
1 Conservative and biomechanical treatment
It is the foundation. It combines cushioning custom insoles designed for cavus foot (as opposed to flatfoot), with bridge padding, selective offloading of metatarsal heads (retrocapital pad, U/donut in painful heads) and, if there is flexible varus, rearfoot valgus wedge. We associate footwear with a wide last and good shock absorption, peroneal and intrinsic musculature strengthening, proprioception work to reduce lateral ankle instability and, if there are incipient claw toes, digital silicone orthoses. This approach resolves or stabilizes a substantial majority of patients for years.
2 Treatment of associated pathologies
Before considering major cavus surgery, symptomatic associated pathologies should be resolved: metatarsalgia (with retrocapital pad and appropriate insole), atypical plantar fasciitis, peroneal tendinopathy, painful plantar calluses (with regular chiropody). In many cases, by treating the associated conditions well, the patient is functionally well without the need to operate on the main bony deformity.
3 MIS forefoot surgery
In patients with pain refractory to conservative treatment, painful claw toes, disabling metatarsalgia or symptomatic forefoot equinus, minimally invasive surgery offers powerful options: dorsal osteotomy of the first metatarsal (percutaneous closing wedge) to correct the equinus and unload the forefoot, percutaneous tenotomies of the flexors in claw toes, selective plantar fasciotomy and, when necessary, percutaneous lengthening of the Achilles tendon. Outpatient surgery, with local anesthesia, immediate standing with post-surgical shoe and return to normal footwear in 2-4 weeks.
4 Reconstructive surgery (rigid or neurological cases)
In rigid cavus feet, major or progressive deformities (Charcot-Marie-Tooth with evolution), surgery moves on to more complex procedures: Dwyer calcaneal osteotomy (lateralizing to correct rearfoot varus), tendon transfers (posterior tibial to dorsal to correct foot drop in CMT) and, in very advanced cases with subtalar arthrosis, selective triple arthrodesis. These procedures require a period of immobilization, prolonged rehabilitation and are coordinated with the referral orthopedic surgery and traumatology service. In neurological conditions, also with neurology.

Comparison of cavus foot treatments
| Criteria | Cushioning insole | Treatment of associated pathologies | MIS forefoot surgery | Reconstructive surgery |
|---|---|---|---|---|
| Indication | Flexible symptomatic cavus foot, first line | Metatarsalgia, mild claw toes, plantar fasciitis | Refractory, painful claw toes, forefoot equinus | Stiff cavus foot, progressive neurological, osteoarthritis |
| Invasiveness | Null | Minimal | Millimeter incisions (mm) | Open or combined surgery |
| Recovery | Adaptation 1-2 wk | Variable | Post-surgical shoe, normal footwear 2-4 wk | Immobilization 6-8 wk, rehab 4-6 mo. |
| Anesthesia | – | – | Local | Regional or general |
| Coordination | Podiatrist | Podiatrist + physiotherapy | Podiatrist MIS | Traumatology + neurology if applicable |
Source: Ortiz C, Wagner E. JBJS Rev 2017; Maskill MP et al. Foot Ankle Int 2010; Manoli A 2nd, Graham B. Foot Ankle Int 2005. Individual results may vary.
Advantages of MIS forefoot surgery in cavus feet
Immediate bipedestation
You walk the same day with a post-surgical forefoot off-loading shoe, no cast, no hospitalization.
Local anesthesia
Without general anesthesia in the vast majority of cases, without prolonged fasting, greater safety.
Millimeter incisions
Multiple surgical procedures (osteotomy, tenotomy, fasciotomy) with several incisions of a few millimeters. Aesthetic result far superior to open surgery.
Forefoot correction
Lowers the forefoot equinus, redistributes loads and relieves metatarsalgia without plaster or bulky internal fixation.
Compatible with major surgery
If calcaneal osteotomy or arthrodesis is required in the future, previous MIS procedures do not hinder it.
Faster recovery
Return to normal footwear in 2-4 weeks and to impact sports in 10-14 weeks, significantly faster than traditional open surgery.
Maintenance and life with cavus foot
The cavus foot requires lifelong follow-up, especially when there is neurological substrate. These three levers summarize the maintenance plan:
👟 Footwear and insole
Shoes with a wide last (especially in the forefoot), good rear and forefoot cushioning, removable insole to use the customized one. Renewal of sports shoes every 600-800 km. High boot with good ankle support in patients with lateral instability or recurrent sprains.
🦵 Proprioception and strength
Daily proprioception work on unstable surfaces (Freeman plate, bosu), peroneal strengthening with elastic bands, daily stretching of the triceps suralis and intrinsic musculature. In patients with Charcot-Marie-Tooth, exercises adapted and guided by neurology and physiotherapy.
📅 Periodic review
Podiatric check-up every 6-12 months in symptomatic cavus feet. In progressive neurological cavus feet, joint follow-up with neurology and, according to evolution, more frequent check-ups to detect early worsening. Renewal of insole every 12-18 months, earlier if there is evident wear.

Do you have a high arch, frequent sprains or persistent metatarsalgia?
Symptomatic cavus foot has effective treatment. Structured diagnosis to rule out neurological causes, specific shock-absorbing insoles and MIS surgery when appropriate.
Request your free evaluationFrequently asked questions about cavus feet
We solve the most common doubts of our patients and families.
🔬 About the pathology.
What is cavus foot?
The cavus foot is the opposite of the flatfoot: the internal longitudinal arch is exaggeratedly high, the rearfoot is usually in varus and the forefoot is in fixed plantar flexion. The result is a stiff foot, with poor shock absorption capacity, which supports load mainly on the heel and metatarsal heads, leaving almost the entire midfoot in the air. This abnormal distribution causes metatarsalgia, claw toes, recurrent ankle sprains and calluses.
Why does cavus foot appear?
In a significant proportion of cases, cavus feet have an underlying neurological cause: the most frequent is Charcot-Marie-Tooth disease, followed by hereditary ataxias, sequelae of poliomyelitis, spina bifida or spinal cord injury. There are idiopathic cavus feet with no identifiable cause. Therefore, when faced with a bilateral, symmetrical and progressive cavus foot, especially in children or adolescents, a neurological evaluation is always advisable.
Is it the same as supinator foot?
They are related but not identical concepts. Supination is the functional position of the foot that rotates outward. The cavus foot is a structural deformity. Almost all cavus feet are supinated, but not all functional supinator feet are structural cavus. The difference matters for diagnosis: structural cavus foot requires specific approach (shock absorbing insole, not just lateral post).
My child has a very high arch: is there anything to worry about?
A slightly higher than average arch may be a normal variant without clinical repercussions. But a progressive cavus foot in a child or adolescent, especially bilateral and symmetrical, with clumsiness in running, frequent falls or repeated sprains, warrants podiatric and almost always neurological assessment. Early detection changes the prognosis because it allows the deformity to be treated while it is still flexible.
🦶 Associated symptoms
What are the most frequent associated problems?
Due to abnormal load distribution, the cavus foot is associated with: metatarsalgia and metatarsal head calluses, claw toes, sesamoiditis, plantar fasciitis, peroneal tendinopathy, recurrent ankle sprains, stress fractures of the 5th metatarsal and low back pain due to postural decompensation. Identifying and treating the associated pathologies usually relieves the patient more than focusing exclusively on the arch.
I sprain my ankle all the time: does it have to do with my cavus foot?
Almost certainly yes. The cavus foot with hindfoot varus places the ankle in a position of mechanical instability: the calcaneus tends to invert and any irregularity of the terrain causes sprain. This is one of the most recognizable clinical scenarios of cavus foot. Treatment begins with insoles with a valgus wedge and peroneal strengthening. If they persist, surgery is considered.
🏥 Treatment
Do insoles work in cavus foot?
Yes, and they are the first line in symptomatic flexible cavus feet. A well-designed cavus foot insole is not the same as a flatfoot insole: it incorporates generous cushioning, selective offloading of metatarsal heads, transverse anterior arch support and rearfoot valgus wedge if flexible varus is present. They reduce metatarsalgia, improve ankle stability and usually keep the patient active for years without surgery.
What does MIS cavus foot surgery consist of?
The surgical approach depends on the type and stiffness of the cavus foot. Minimally invasive surgery allows several components to be operated on with millimeter incisions: dorsal osteotomy of the first metatarsal to correct the equinus, percutaneous tenotomies of the flexors in claw toes and, when necessary, plantar fasciotomy. MIS surgery does not replace major bony procedures when necessary, but allows resolution of the forefoot component with immediate standing.
Is it always necessary to operate?
No. A significant proportion of cavus foot patients are managed for years or decades with conservative treatment. Surgery is considered when there is persistent pain, disabling metatarsalgia, refractory painful claw toes, lateral ankle instability with recurrent sprains or, in progressive neurological cavus feet, before the deformity becomes rigid. The decision is individual.
Does surgery solve cavus foot forever?
It depends on the cause. In stable idiopathic cavus foot, a well indicated surgery can maintain results for many years. In progressive neurological cavus feet (especially Charcot-Marie-Tooth), surgery corrects the current deformity but the underlying disease may continue to evolve, so joint follow-up with neurology is essential.
Scientific references
- Ortiz C, Wagner E. Diagnosis and treatment of cavus foot. JBJS Rev. 2017.
- Maskill MP, Maskill JD, Pomeroy GC. Surgical management and treatment algorithm for the subtle cavovarus foot. Foot Ankle Int. 2010;31(12):1057-1063.
- Manoli A 2nd, Graham B. The subtle cavus foot, “the underpronator”. Foot Ankle Int. 2005;26(3):256-263.
- Pfeffer GB, Michalski MP, Basak T, et al. Use of 3D Modeling for Cavovarus Foot Reconstruction. Foot Ankle Int. 2020.
- Bibbo C, Jaglan SS. Percutaneous tenotomies and osteotomies in foot surgery. Clin Podiatr Med Surg. 2018.
- Younger AS, Hansen ST Jr. Adult cavovarus foot. J Am Acad Orthop Surg. 2005;13(5):302-315.
- Pareyson D, Marchesi C. Diagnosis, natural history, and management of Charcot-Marie-Tooth disease. Lancet Neurol. 2009;8(7):654-667.
Information prepared by the medical team of Clínica San Román. Center No. 5357 Autonomous Registry of Health Centers, Services and Establishments of the Valencian Community. This page is for information purposes only and does not replace the individual clinical assessment.
Restores stability and cushioning to your cavus feet
Structured diagnosis, specific insoles, MIS surgery when appropriate and neurological coordination if necessary. 45 years of experience in foot biomechanics.
- 📞 +34 965 921 156
- ✉️ info@clinicasanroman.com
- Av. del Dr. Ramón y Cajal 1, 03001 Alicante