
PREVENTATIVE PODIATRY – DIABETIC FOOT – ALICANTE
Diabetic foot: prevention, monitoring and early action
Screening, therapeutic footwear, customized offloading, safe chiropody and prophylactic MIS surgery when appropriate. All in coordination with your endocrinologist and medical team. 45 years in foot pathology.

45 years of experience in foot pathology
Clinic founded in 1979
Three generations specialized in foot care for patients with chronic pathologies.
Certification MIS23BE03
Accredited by the American Board of Multispecialty Podiatry for minimally invasive surgery of the foot.
Multilingual service
We attend you in Spanish, English, German, French and Dutch.
What is diabetic foot?
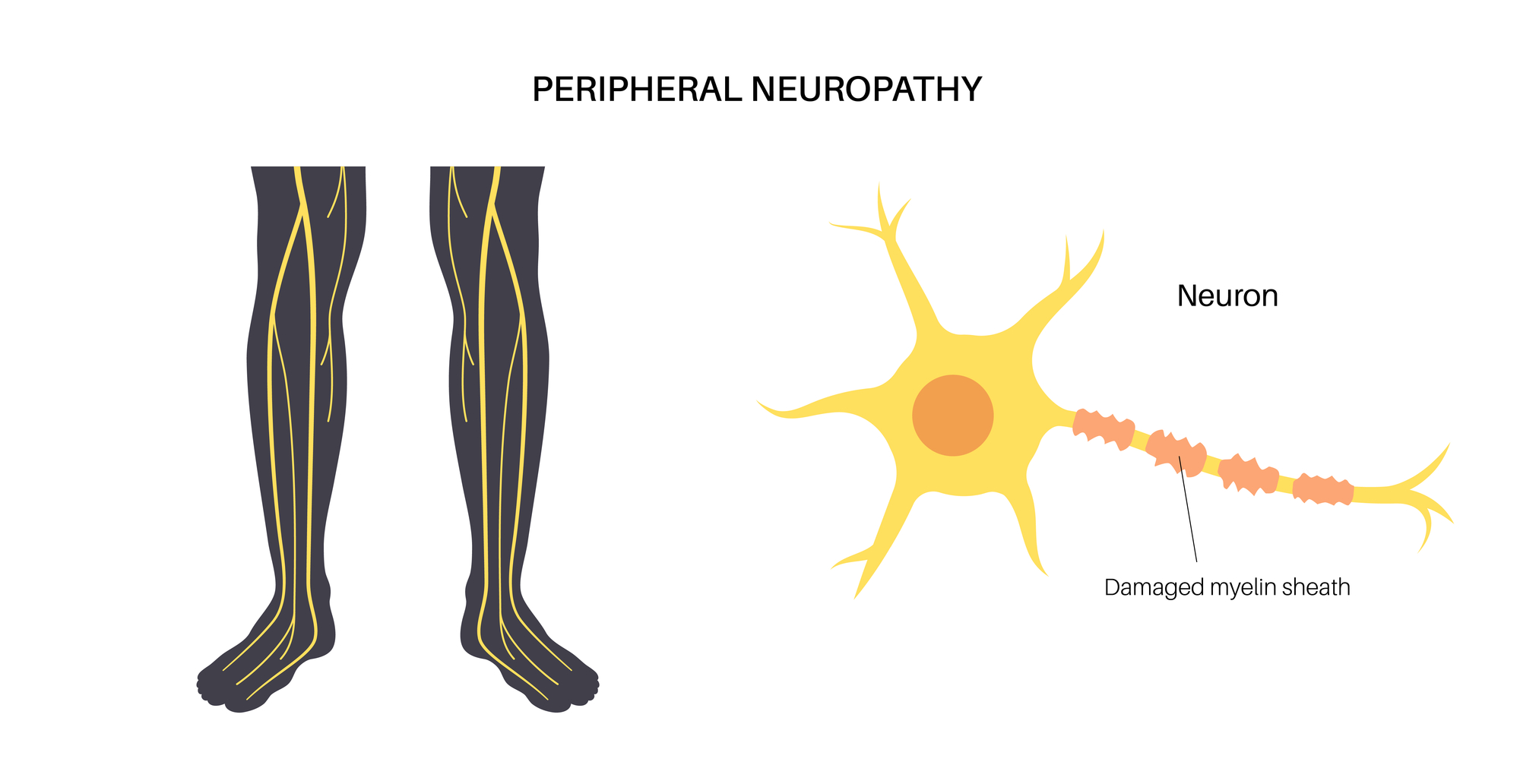
Diabetic foot is not a single disease, but a complex syndrome that encompasses the set of foot complications that can appear in patients with diabetes mellitus over the years. Its root cause combines three elements: diabetic peripheral neuropathy (with loss of protective sensitivity), peripheral arteriopathy (with decreased blood supply) and increased susceptibility to infection.
The combination of these three factors explains why small injuries that would go unnoticed in a person without diabetes – a graze, an ingrown toenail, a callus – can develop into chronic ulcers, serious infections and, in the worst cases, amputations. International guidelines from the International Working Group on the Diabetic Foot (IWGDF) describe the diabetic foot as one of the most costly complications, in human and health terms, of diabetes.
The good news is that a considerable majority of diabetic foot complications are preventable through periodic screening, patient education, proper offloading of hyperpressure areas and, when appropriate, prophylactic minimally invasive surgery to correct ulcer-generating deformities. At Clínica San Román we work in coordination with your primary care physician, your endocrinologist or internist and the vascular surgery and traumatology services of reference, because diabetic foot is approached as a team.
Signs and symptoms: what should you watch for?
The diabetic foot is, to a large extent, a “silent” pathology: many of its most important signs do not produce acute pain, precisely because neuropathy eliminates the alarm signal. This is what justifies daily self-inspection and periodic podiatric screening, even in apparently normal feet.
- Loss of sensitivity to touch, pinprick or temperature in feet or legs.
- Tingling, burning or cramping sensation at night in the lower limbs.
- Dry skin, cracks in heels and pressure areas, thick calluses.
- Color changes (pallor, redness, cyanosis), feet cold to the touch.
- Loss of hair on legs and fingers, skin atrophy.
- Thickened, brittle or discolored nails (suspected onychomycosis).
- Any wound that does not heal within a few days, no matter how small it may seem.
- Swollen, hot and reddened foot without proportional pain (suspicion of acute Charcot or deep infection).
- Progressive deformities: claw toes, bunions, arch collapse.
- Leg pain when walking that improves when stopping (claudication, suspected arteriopathy).
What factors increase the risk of diabetic foot?
The risk is not the same in all patients with diabetes. Identifying and modulating the factors that increase that risk is what makes it possible to build a personalized and effective preventive plan.
🩸 Metabolic control and duration.
Suboptimal glycemic control (sustained elevated HbA1c) and prolonged duration of diabetes are the two main drivers of the development of neuropathy and vasculopathy. Added hypertension, dyslipidemia and smoking increase the risk of cardiovascular and distal complications. Working together with endocrinology, primary care and, if appropriate, cardiology, is the basis for any podiatric strategy.
🦶 Foot at risk (deformities and antecedents)
The presence of foot deformities – claw toes, bunions, bony prominences, forefoot equinus – increases the areas of hyperpressure where an ulcer is likely to form. A history of previous ulceration or amputation significantly multiplies the risk of a new ulcer: once a point of the foot has failed, that point remains vulnerable. Established Charcot foot is a very powerful independent risk factor.
🧦 Habits and self-care.
Inadequate footwear, aggressive stitching, barefoot walking, chemical callicides, too deep nail cuts, lack of daily foot inspection, lack of regular professional chiropody… an important part of diabetic foot ulcers are avoidable with education. SEMERGEN, the Spanish Diabetes Society and the IWGDF guidelines insist on the importance of well-informed self-care as a preventive tool.
Podiatric evaluation of the diabetic foot: how do we screen?
At Clínica San Román we protocolize the assessment of the diabetic patient’s foot following the IWGDF guidelines. The objective is to stratify the risk of each patient and design an adapted follow-up plan, in coordination with the medical team responsible for diabetes.
🧪 Neuropathic screening.
We use simple and well validated tests: Semmes-Weinstein 10 g monofilament at various points on the foot (protective sensitivity), calibrated 128 Hz tuning fork (vibratory sensitivity), assessment of Achilles reflexes and, when appropriate, biotensiometer. The absence of response to the monofilament at any point is already a marker of loss of protective sensitivity and modifies the follow-up plan.
🩺 Vascular assessment
Bilateral palpation of pedial and posterior tibial pulses, exploration of color, temperature, capillary filling and time of pallor when elevating the limb. If arteriopathy is suspected, ankle-brachial index (ABI) with portable Doppler and referral to vascular surgery if necessary. Adequate perfusion is a prerequisite for any surgery or aggressive procedure on the foot.
📊 Biomechanical and pressure studies
Prescan footprint analysis and structured deformity scanning. Identifies areas of hyperpressure where ulceration is most likely to occur and guides the design of off-loading insoles and, when appropriate, the indication for prophylactic MIS surgery.
📋 Risk stratification IWGDF
With all the data we classify the patient in his or her risk group according to the IWGDF system (0-3) and establish the frequency of follow-up, preventive measures and the possible need for therapeutic footwear, unloading insoles or urgent referral. The stratification is dynamic: it is reevaluated at each revision.
Comprehensive diabetic foot program: four levels of action
The treatment of the diabetic foot is, above all, preventive and multidisciplinary. Surgery is reserved for very specific indications and always within a global plan for the control of the underlying disease.
1 Primary prevention and education
It is the cornerstone. It includes education of the patient and their environment (daily self-inspection, hygiene, hydration, footwear), periodic screening with the frequency established by the IWGDF stratification, safe and regular chiropody performed by a podiatrist (nail trimming, controlled delamination of calluses, without chemical aggression), recommendations for appropriate footwear and, when appropriate, personalized insole that distributes pressure and protects risk areas. At this level we coordinate closely with your diabetes physician.
2 Established foot at risk: unloading and therapeutic footwear
In patients with established neuropathy and/or deformity, without active ulceration but with clear risk, we escalate to custom insoles designed from the pressure study, therapeutic footwear (wide and deep last, rigid sole with rocker, firm buttress, no aggressive internal seams) and, if there are digital deformities, protective silicone orthoses. Check-ups are intensified (every 3-6 months depending on the case). The objective is clear: to avoid the first ulcer.
3 Prophylactic MIS surgery in selected cases
In patients with good metabolic control, adequate vascular perfusion and specific deformities that generate recurrent hyperpressure(claw toes, plantar exostoses, forefoot equinus, bunions) that have caused previous ulceration or are at clear risk of doing so, prophylactic minimally invasive surgery can play an important role. We are talking about percutaneous osteotomies and tenotomies with millimetric incisions, local anesthesia, ambulatory, which unload the area of hyperpressure and reduce the risk of future ulceration. The indication is decided on a case-by-case basis, within the multidisciplinary program, and never as an isolated solution.
4 Management of active ulcer and major reconstruction
In the case of an active ulcer, the approach requires coordination with the multidisciplinary diabetic foot unit of the health system: strict offloading (total offloading boot or total contact cast when appropriate), specialized local dressings, assessment and treatment of infection if present, urgent vascular assessment and strict metabolic control. In established Charcot foot or complex ulcers with bone involvement (osteomyelitis), major reconstructive surgery is planned jointly with traumatology, vascular surgery and the medical unit responsible for diabetes. Our role here is one of close podiatric follow-up within the team.

Risk stratification and frequency of review (based on IWGDF)
| Risk group | Characteristics | Frequency of podiatric examination | Preventive measures |
|---|---|---|---|
| Group 0 | No neuropathy, no vasculopathy | Annual screening | Education, proper footwear, self-inspection |
| Group 1 | Neuropathy without deformity or previous ulceration | Every 6-12 months | Appropriate footwear, insole if appropriate, regular chiropody |
| Group 2 | Neuropathy + deformity and/or vasculopathy | Every 3-6 months | Relief insole, therapeutic footwear, assessment of prophylactic MIS surgery |
| Group 3 | Previous ulcer or amputation | Every 1-3 months | Mandatory therapeutic footwear, custom-made insole, active surveillance |
Adapted from IWGDF Guidelines 2023 (Schaper NC et al.). Specific frequencies are agreed upon by your medical team based on your individual clinical situation.
Why follow your diabetic foot at Clínica San Román?
Structured screening IWGDF
Standardized examination with monofilament, tuning fork, pulse palpation and, when appropriate, ITB. Risk stratification at each visit.
Insoles and therapeutic footwear
Custom insoles based on pressure studies. Guidance on therapeutic footwear when necessary.
Safe chiropody
Nail trimming and controlled delamination of calluses on insensitive skin. No chemical aggression, no risk of inadvertent micro-injury.
Prophylactic MIS surgery
Percutaneous osteotomies and tenotomies in selected cases to relieve areas of hyperpressure and reduce ulcer risk.
Multidisciplinary coordination
Teamwork with your endocrinologist, primary care physician, vascular surgery and traumatology. Shared information and common plan.
Patient education
Clear self-care program: daily inspection, footwear, hygiene, warning signs. Material adapted to each risk profile.
Ten keys to diabetic foot self-care
These are the basic recommendations we make to our diabetic patients and are aligned with the IWGDF and Spanish Diabetes Society guidelines:
👀 Inspection and hygiene
Inspect your feet every day, including the soles and spaces between the toes (use a mirror if necessary). Wash with lukewarm (not hot) water, dry well, especially between the toes. Moisturize with cream on the instep and soles, avoiding the interdigital spaces. In case of any wound, crack, callus or change of color, consult without delay.
👟 Footwear and insole
Shoes with a wide last, sufficient depth, rigid sole with good cushioning, without aggressive internal stitching. Inspect the inside before putting on your shoes (pebbles, objects, displaced seams). Do not go barefoot, even at home or at the beach. Wear socks or stockings of natural fiber, without excessive compression. If you have a personalized insole, always use it.
✂️ Nails and calluses
Cut the nails in a straight line, without deepening the edges, with nail clippers with good vision. Do not use razors or chemical callicides (keratolytics, bunion patches with salicylic acid): they can cause severe chemical burns on insensitive skin. Painful or thick calluses are treated by a podiatrist. Go for professional chiropody as often as indicated.

Have you not had your foot appraised for more than a year?
If you have diabetes – type 1 or type 2 – annual screening is not optional. Ten minutes of screening can make the difference between years without complications and a complicated ulcer. We talk to your medical team to coordinate follow-up.
Request your free evaluationFrequently asked questions about the diabetic foot
We solve the most common questions that our diabetic patients and their families ask us in consultation.
🔬 About the pathology.
What is diabetic foot?
It is a complex syndrome, not a single disease. It encompasses the foot complications that can appear in patients with diabetes mellitus over the years. Its root cause combines three elements: diabetic neuropathy (loss of protective sensation), peripheral arteriopathy (decreased blood supply) and increased susceptibility to infection. The combination of the three explains why small lesions can evolve into chronic ulcers.
Why are diabetic foot ulcers so dangerous?
By the combination of three factors. First, neuropathy causes the patient not to perceive the lesion. Second, arteriopathy limits the blood supply necessary for healing. Third, relative immunosuppression facilitates infection. The result is that a banal wound can progress in days to a deep ulcer, reach the bone (osteomyelitis) and compromise the viability of the foot. That is why any wound should be assessed as soon as possible.
What is Charcot foot?
Charcot neuroarthropathy is a severe and often underdiagnosed complication of neuropathic diabetic foot. It consists of progressive bone and joint destruction, usually of the midfoot. The acute picture presents with a hot, swollen and erythematous foot – often mistaken for cellulitis or venous thrombosis – but typically without commensurate pain. Without early diagnosis, it progresses to severe bone deformity and high risk of amputation. Urgent referral for a hot, deformed diabetic foot.
How is diabetic foot neuropathy detected?
In consultation we use validated tests: Semmes-Weinstein 10 g monofilament (protective sensitivity), 128 Hz calibrated tuning fork (vibratory sensitivity) and assessment of Achilles reflexes. We complement with palpation of pedial and posterior tibial pulses, ankle-brachial index and, if necessary, neurophysiological study. Early detection of loss of protective sensitivity changes the follow-up and reduces the risk of future ulceration.
🏥 Treatment and follow-up
I am diabetic: how often do I have to see a podiatrist?
It depends on the risk level of your foot. In a foot without neuropathy or vasculopathy (group 0 IWGDF), annual screening. With neuropathy without deformity (group 1), every 6-12 months. With neuropathy and deformity or vasculopathy (group 2), every 3-6 months. With a history of ulcer or amputation (group 3), every 1-3 months. Minimum annual screening in every diabetic patient is not optional. Your medical team sets the exact frequency.
Can a diabetic ulcer be cured?
Yes, most of them close with adequate treatment, although the path requires perseverance. The mainstay is strict offloading of the ulcer: total offloading boot or total contact cast (TCC) in selected cases, both validated as gold standard by international guidelines. They are accompanied by specialized local dressings, assessment and treatment of infection, vascular assessment and optimal metabolic control. Healing requires weeks or months depending on the case. Recurrence is high, so subsequent prevention is critical.
Does minimally invasive surgery have a role in the diabetic foot?
Yes, and increasingly important. Prophylactic surgery of the diabetic foot uses percutaneous osteotomies and tenotomies to correct hyperpressure-generating deformities and thus prevent future ulcers or help close refractory ulcers. The indication must be carefully selected: patient with good metabolic control, adequate vascular perfusion and within a multidisciplinary program. It is not for all diabetic feet.
Who should treat my diabetic foot?
The correct approach to the diabetic foot is multidisciplinary. International guidelines recommend organizing care around a unit or circuit that coordinates: your primary care physician, your endocrinologist or internist, the specialist podiatrist, the vascular surgeon (when arteriopathy is present) and the orthopedic surgeon/traumatologist (in major surgery or Charcot foot). No professional acts in isolation in cases of foot at risk.
🧦 Self-care
Can I cut my nails or remove calluses at home?
It is one of the areas where most damage is prevented. In a patient with neuropathy, home chiropody is a frequent source of injury. Cut the nails in a straight line, without deepening the edges. Never use blades or chemical callicides: they can generate severe chemical burns on insensitive skin. Painful or thick calluses are treated by a podiatrist. If you have any doubts, consult before acting.
What footwear should I wear?
Wide last (especially in the forefoot), sufficient depth to accommodate insole, rigid sole with good cushioning, firm counter, absence of aggressive internal seams, flexible material in the instep. In patients with neuropathy and deformity, specific therapeutic footwear with customized insole. Before putting on your shoes, inspect the inside. Daily inspection of the feet, especially between the toes.
Scientific references
- Schaper NC, van Netten JJ, Apelqvist J, et al. Practical guidelines on the prevention and management of diabetes-related foot disease (IWGDF 2023 update). Diabetes Metab Res Rev. 2023.
- Armstrong DG, Boulton AJM, Bus SA. Diabetic Foot Ulcers and Their Recurrence. N Engl J Med. 2017;376(24):2367-2375.
- Boulton AJM, Armstrong DG, Kirsner RS, et al. Diagnosis and Management of Diabetic Foot Complications. American Diabetes Association. 2018.
- Lázaro-Martínez JL, Aragón-Sánchez J, García-Morales E. Antibiotics versus conservative surgery for treating diabetic foot osteomyelitis. Diabetes Care. 2014;37(3):789-795.
- Frykberg RG, Bevilacqua NJ, Habershaw G. Surgical off-loading of the diabetic foot. J Vasc Surg. 2010;52(3 Suppl):44S-58S.
- Boulton AJM. The diabetic foot. Med Clin North Am. 2013;97(5):775-790.
- Spanish Diabetes Society (SED). Clinical guidelines on diabetes. Last update available at sediabetes.org.
Information prepared by the medical team of Clínica San Román. Center number 5357 Autonomous Registry of Health Centers, Services and Establishments of the Valencian Community. This page is for information purposes only and does not replace the individual clinical assessment. If you have diabetes, follow the instructions of your medical team (primary care, endocrinology, vascular surgery and diabetic foot unit when appropriate). Go to the emergency room for any wound or injury to the foot that requires immediate attention.
Take care of your diabetic foot today so you won’t regret it tomorrow.
Periodic screening, custom insoles, therapeutic footwear, safe chiropody and prophylactic MIS surgery when appropriate. All in coordination with your diabetes medical team.
- 📞 +34 965 921 156
- ✉️ info@clinicasanroman.com
- Av. del Dr. Ramón y Cajal 1, 03001 Alicante