
PODIATRY – BIOMECHANICS – SURGERY MY – ALICANTE
Valgus foot treatment: corrects heel alignment without loss of quality of life
Pediatric and adult hindfoot valgus staging protocol. Biomechanical insoles and MIS arthroereisis when appropriate. Correcting footprint since 1979 in Alicante.

Correcting footprint since 1979 in Alicante
Clinic founded in 1979
Specialists since 1979 in foot biomechanics for children, adults and athletes.
Certification MIS23BE03
Accredited by the American Board of Multispecialty Podiatry for minimally invasive surgery.
Multilingual service
We attend you in Spanish, English, German, French and Dutch.
What is valgus foot?
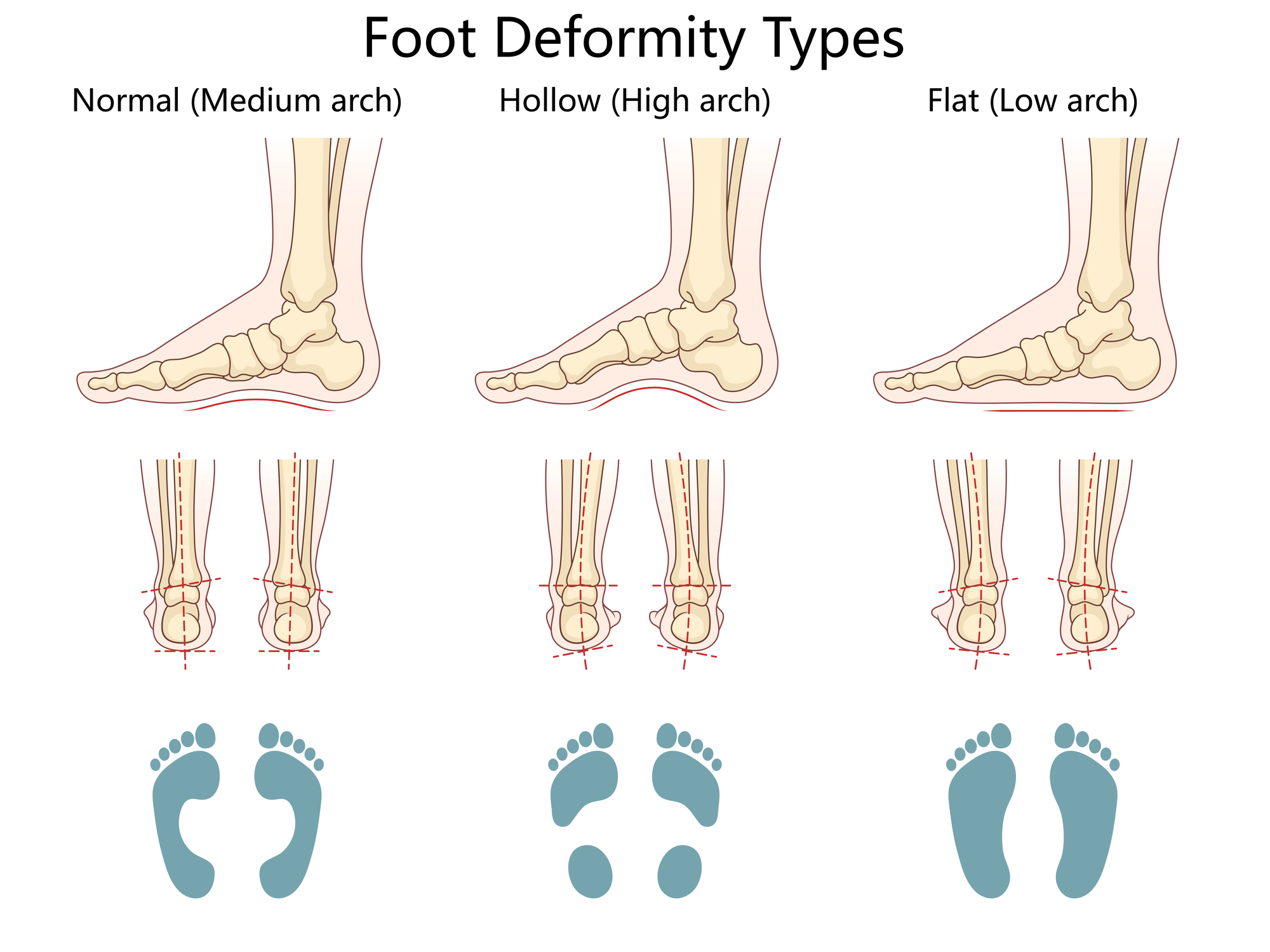
Valgus foot is an alteration of the rearfoot axis in which the calcaneus is inverted with respect to the longitudinal axis of the tibia (falls towards the medial plane of the body). Seen from behind, the heel tilts inward and the internal arch tends to flatten. When this valgus is accompanied by internal longitudinal arch subsidence and forefoot abduction, we speak of flatfoot-valgus or, more correctly, pronator foot: the biomechanical pattern we see in the vast majority of patients with problems associated with excessive pronation.
In children, some valgus is physiological until the age of 4-6 years: the foot is maturing and learning to stabilize itself during walking. The vast majority resolve on their own. In adults, valgus foot that appears or progresses after the age of 40 is usually secondary to dysfunction of the posterior tibial tendon, the main dynamic stabilizer of the subtalar joint, and is staged as adult acquired flatfoot.
At Clínica San Román we approach valgus foot as a correctable biomechanical alteration: minimum necessary treatment, staggered from custom insoles to minimally invasive subtalar arthroereisis, reserving regular open surgery for advanced cases in collaboration with traumatology.
Symptoms: when does a valgus foot need treatment?
Asymptomatic valgus foot does not require aggressive treatment; valgus foot that hurts, fatigues or impacts gait does. These are the signs that warrant professional assessment:
- Visible heel emersion when observing the patient from behind (calcaneus tilted towards the midline).
- Falling of the internal arch in standing position, with normalization when standing on tiptoe.
- Sign of the many visible toes: three or more toes protrude outside the heel when viewed from behind (instead of one or two).
- Asymmetrical wear of the shoe at the inner edge of the heel or inner forefoot of the sole.
- Pain or fatigue in the medial aspect of the ankle and posterior tibial tendon area after prolonged walking.
- Anterior or medial knee pain due to decompensation of the ascending kinetic chain.
- Frequent falls in children, clumsy gait, fatigue when walking more than 30-45 minutes.
- Night cramps in calf muscles, overload of posterior leg muscles.
Why does valgus foot appear?
Hindfoot valgus is the result of a disproportion between the forces that evvert the calcaneus (calcaneus, peroneals, body weight in pronation) and those that supinate it (posterior tibialis, spring ligament, intrinsics). Identifying which predominates determines effective treatment.
👶 Pediatric factors.
Generalized ligamentous laxity (frequent, hereditary) is the most common cause of flexible valgus in children. Child overweight, early gait without balance training, cerebral palsy and, in rigid conditions, tarsal coalitions are the pathological causes to be ruled out. The vast majority of pediatric valgus are flexible, physiological and self-resolving with development.
🦶 Posterior tibial dysfunction
It is the most common cause of adult acquired valgus. The tibialis posterior is the main dynamic supinator of the rearfoot. Its weakness, tendinopathy or rupture allows the calcaneus to be progressively inverted. It typically appears between 40 and 60 years of age, with a predilection for women, overweight, hypertension and diabetes. Without treatment it progresses by stages (Johnson-Strom I-IV).
⚖️ Overload and global biomechanics
Overweight, prolonged standing, flat non-restrained footwear and triceps suralis (ankle equinus) stiffness are factors that accelerate any underlying valgus. Lower limb dysmetria and associated genu valgum amplify pronation. Biomechanics never occurs in a vacuum: it is affected by the entire kinetic chain.
Diagnosis: how do we evaluate hindfoot valgus?
A good diagnosis of valgus foot requires measuring, not estimating. At Clínica San Román we protocolize the assessment in four complementary levels that allow us to differentiate flexible/rigid, physiological/pathological and plan effective treatment.
🔍 Clinical examination of the calcaneal-tibial axis.
We assess the patient in standing with bilateral support, gait and dynamic tests. We measure the calcaneal-tibial angle in posterior vision, we apply the sign of the many visible toes, the Jack test (elevation of the first toe: the arch must be formed), the single heel rise (tiptoe with only one foot: altered in DTTP) and we evaluate the reducibility of the valgus in seated position.
📊 Computerized biomechanical analysis
Gait analysis on prescanner and, when appropriate, force platform and gait video. Objectively documents degree of pronation, asymmetries between both feet, toe-off phase, peak pressures and areas of overload. Provides objective evidence before and after treatment.
📷 Bilateral loading radiography
Dorsoplantar, lateral loading and axial calcaneal projection. It measures the Costa-Bertani angle (medial), the Meary-Tomeno angle, the calcaneal inclination angle and the talus-scaphoid coverage. It detects bony coalitions, signs of subtalar arthrosis and associated deformities. The loading radiograph is the only one that provides real biomechanical information.
🔊 Ultrasound and magnetic resonance imaging
In adults with suspected tibialis posterior dysfunction, dynamic ultrasound assesses integrity, continuity and peritendinous effusion. MRI is the gold standard for staging tendinopathy or rupture, assessing spring ligament injuries and planning surgery when appropriate. It is reserved for cases refractory to conservative treatment.
Treatment of valgus foot: stepwise protocol
The vast majority of valgus feet are controlled with conservative treatment. Surgery is reserved for refractory cases or advanced stages, and we always start with the least invasive approach.
1 Conservative and biomechanical treatment
This is the basis of the protocol. It combines custom insole with medial calcaneal post and supinator wedge adjusted to the degree of valgus, footwear with rearfoot containment and stable last, specific physiotherapy (posterior tibial strengthening with eccentric exercises, intrinsic foot supinators, triceps sural stretching) and gait education. In the child with symptomatic valgus, it avoids overload; in adult stage I PTTP, this approach resolves or stabilizes a considerable majority of patients at 3-6 months.
2 Rigid orthoses and adjuvant work
When the standard insole does not achieve the expected control after 3-6 months in stage II adults, we escalate to Arizona-type rigid orthoses (wraparound, semi-rigid) or UCBL to stabilize the hindfoot more actively. We associate ultrasound-guided infiltration of the posterior tibial with PRP or selective corticosteroid when there is tendinopathy or frank tenosynovitis. These measures can maintain the patient without progression for years and, in many cases, avoid surgery.
3 Subtalar MIS subtalar arthroereisis
In symptomatic flexible valgus feet refractory to conservative treatment -both in selected pediatric (typically from 9-12 years of age) and adult stage II flexible feet-, minimally invasive subtalar arthroereisis is an effective alternative. Percutaneous implantation in the sinus of the tarsus through a millimeter incision under local or regional anesthesia. Limits pronation, corrects valgus and restores arch. Immediate ambulation with walker boot, return to light activity 2-4 weeks and sport 10-14 weeks. The implant is reversible if it loses indication in the future.
4 Reconstructive surgery (advanced stages)
In adult rigid valgus, stages III-IV of acquired flatfoot or pediatric cases with symptomatic tarsal coalition, surgery moves to reconstructive procedures: medializing calcaneal osteotomy, transfer of flexor digitorum longus to posterior tibialis, lateral column lengthening and, in very advanced stages with subtalar arthrosis, selective arthrodesis. These procedures require a longer period of immobilization and rehabilitation. The indication is coordinated with the referral orthopedic surgery and traumatology service.

Comparison of valgus foot treatments
| Criteria | Personalized insole | Arizona Orthosis + infiltration | MIS arthroereisis | Calcaneal osteotomy |
|---|---|---|---|---|
| Indication | Symptomatic flexible valgus, child and adult stage I | Stage II flexible with DTTP, template failure | Refractory flexible, pediatric and adult | Rigid valgus, MIS failure, major deformity |
| Invasiveness | Null | Minimal | Percutaneous incision (mm) | Open calcaneal surgery |
| Recovery | Adaptation 1-2 weeks | Spaced sessions | Immediate standing, sport 10-14 wk. | Immobilization 6-8 wks, prolonged rehab |
| Reversibility | Total | Total | Removable implant | Definitive |
| Pediatric indication | Yes, first line | Not usual | Yes, in selected cases | Exceptional, coordinated with pediatric traumatology |
Source: Johnson KA, Strom DE. Clin Orthop 1989; Vora AM et al. JBJS 2006; Bouchard M, Mosca VS. JAAOS 2014. Individual results may vary.
Advantages of MIS arthroereisis of valgus foot
Immediate bipedestation
You walk the same day with a walker boot or post-surgical shoe, no cast, no admission.
Local or regional anesthesia
No general anesthesia in most cases, no prolonged fasting, greater safety.
Millimeter incision
Almost imperceptible scar. Aesthetic result far superior to open surgery of the calcaneus.
Reversible
The implant may be removed in the future if it loses indication or discomfort appears.
Does not burn bridges
If major reconstructive surgery is required in the future, prior arthroereisis does not preclude it.
Real biomechanical correction
Documented improvement in radiographic angles and tread pattern in postoperative prescan.
Maintenance and life with controlled valgus foot
Once the symptomatic episode is resolved, maintenance is what sustains the outcome. Three basic levers:
👟 Footwear and insole
Everyday footwear with good rearfoot containment, stable sole, removable insole to use the customized one. Renewal of sports shoes every 600-800 km. Avoid long days with flat shoes without support in patients with symptomatic valgus.
🦵 Supinator strength
Targeted work of the tibialis posterior (eccentric exercises), intrinsic musculature of the foot (short foot exercise), daily stretching of the triceps suralis and proprioception work on unstable surfaces. Five to ten minutes a day will slow down progression.
⚖️ Weight and revision
Body weight control: each extra kilogram increases pronation. Podiatric check-up every 12-18 months in symptomatic adults and annually in pediatric patients until growth is consolidated. After surgery, scheduled check-ups at 3, 6 and 12 months.

Do you suspect that you or your child has symptomatic pes valgus?
We differentiate the physiological from the pathological, accurately measure the hindfoot axis and design a plan adapted to the age and stage. Most valgus feet are controlled without surgery.
Request your free evaluationFrequently asked questions about valgus foot
We solve the most common doubts of our patients and their families.
🔬 About the pathology.
Is valgus foot the same as flatfoot?
No, although they frequently coexist. Valgus foot refers to alignment: the heel is inverted. Flatfoot refers to the arch: the internal longitudinal arch is collapsed. The vast majority of flatfeet are also valgus and vice versa, forming the so-called flatfoot-valgus or pronator foot. But there are flatfeet with preserved arch (typically in children) and flatfeet with discrete valgus. Distinguishing between them is important because the emphasis of treatment varies.
At what age is a valgus foot in a child considered pathological?
Up to the age of 4-6 years, a certain degree of valgus is physiological. After that age, if the valgus persists (more than 7-10° clinical), if it is asymmetrical between the two feet, if it is accompanied by pain or fatigue when walking, or if it limits the child’s activity, a podiatric evaluation is recommended. Most asymptomatic pediatric valgus correct themselves with growth. Pediatric surgery is rare.
What problems can an untreated valgus foot cause?
The valgus foot decompensates the ascending kinetic chain. Excessive pronation of the rearfoot drags the tibia in internal rotation, the patella in lateral overload and the hip in adduction, generating anterior knee pain, patellar tendinopathy, overload of the posterior tibialis and Achilles, pain in the external aspect of the hip and low lumbar overload. In the foot, it favors bunions, claw toes and plantar fasciitis.
What if I have an adult foot?
In adults, persistent or de novo valgus foot is usually associated with posterior tibial tendon dysfunction and is staged as adult acquired flatfoot (Johnson-Strom). Treatment is stage-dependent: insoles and rehabilitation in stage I, Arizona-type orthoses or MIS arthroereisis in stage II flexible, and regimented reconstruction in advanced stages.
🏥 Treatment
Do insoles correct hindfoot valgus?
They control it functionally, not correct it anatomically. A well-designed insole, with a medial calcaneal post and supinator wedge adjusted to the degree of valgus, returns the calcaneus to neutral alignment during gait, reduces posterior tibial overload and normalizes the kinetic chain. It is the first line of treatment and resolves or stabilizes most symptomatic conditions.
What does subtalar arthroereisis consist of?
It is a minimally invasive technique in which a small implant is inserted into the sinus of the tarsus through a percutaneous incision of a few millimeters. The implant acts as a mechanical stop that limits excessive pronation, correcting the valgus and restoring the arch. It is performed under local or regional anesthesia, on an outpatient basis. It is a reasonable alternative in flexible valgus feet refractory to conservative treatment.
Is arthroereisis the same as calcaneal osteotomy?
No. Arthroereisis is percutaneous, minimally invasive, reversible and is indicated in flexible valgus feet. Medializing calcaneal osteotomy is a more complex, definitive open surgery, with a longer immobilization period, and is reserved for rigid cases, important valgus or advanced stages of adult acquired flatfoot. The decision depends on age, grade, stiffness and associated pathology.
How long does recovery take after arthroereisis?
Immediate bipedestation with walker boot or post-surgical shoe from the same day. Reintroduction of normal footwear with insole at 2-3 weeks, light activity at 4-6 weeks and impact sports at 10-14 weeks, with intermediate clinical review. The millimetric scar is practically imperceptible after a few months.
👶 Pediatric specific care.
My child has inward curved heels: do I need surgery?
Not at entry. In the vast majority of cases, pediatric valgus is resolved with observation, appropriate footwear and, if there is symptomatology, insoles. Pediatric valgus surgery is exceptional and is only considered when there is persistent pain or functional limitation after months of conservative treatment, generally from 9-12 years of age. A reasonable first step is podiatric assessment.
What if the valgus returns?
Without treatment, adult valgus foot tends to progress slowly over time, especially in patients with overweight, hypertension or established tibialis posterior dysfunction. That is why clinical discharge always includes a maintenance plan: customized insole, strengthening program and annual check-up. After well-indicated arthroereisis, recurrence of the original condition is rare.
Scientific references
- Johnson KA, Strom DE. Tibialis posterior tendon dysfunction. Clin Orthop Relat Res. 1989;239:196-206.
- Vora AM, Tien TR, Parks BG, et al. Correction of moderate and severe acquired flexible flatfoot. J Bone Joint Surg Am. 2006;88(8):1726-1734.
- Bouchard M, Mosca VS. Flatfoot deformity in children and adolescents: surgical indications and management. J Am Acad Orthop Surg. 2014;22(10):623-632.
- Mosca VS. Flexible flatfoot in children and adolescents. J Child Orthop. 2010;4(2):107-121.
- Kohls-Gatzoulis J, Angel JC, Singh D, et al. Tibialis posterior dysfunction. BMJ. 2004;329(7478):1328-1333.
- Highlander P, May J, Stewart J. The Subtalar Arthroereisis for Flexible Flatfoot. Clin Podiatr Med Surg. 2014;31(3):385-394.
- Cao L, Miao XD, Wang AG, et al. Subtalar arthroereisis for flexible pediatric pes planovalgus. Orthop Surg. 2019;11(1):26-31.
Information prepared by the medical team of Clínica San Román. Center No. 5357 Autonomous Registry of Health Centers, Services and Establishments of the Valencian Community. This page is for information purposes only and does not replace the individual clinical assessment.
Corrects the footprint from the rearfoot
Biomechanical diagnosis, custom insoles, MIS arthroereisis where appropriate. We have been correcting valgus feet in Alicante since 1979.
- 📞 +34 965 921 156
- ✉️ info@clinicasanroman.com
- Av. del Dr. Ramón y Cajal 1, 03001 Alicante