
PODIATRY – BIOMECHANICS – SURGERY MY – ALICANTE
Treatment of flatfoot: from plantar support to MIS arthroereisis
Step protocol for pediatric and adult acquired flatfoot. Accurate biomechanical diagnosis, custom insoles and minimally invasive surgery when appropriate. Specialists since 1979 in foot biomechanics.

Clinical biomechanics since 1979 in Alicante
Clinic founded in 1979
Specialists since 1979 in foot pathology of children, adults and athletes.
Certification MIS23BE03
Accredited by the American Board of Multispecialty Podiatry for minimally invasive surgery.
Multilingual service
We attend you in Spanish, English, German, French and Dutch.
What is flatfoot?
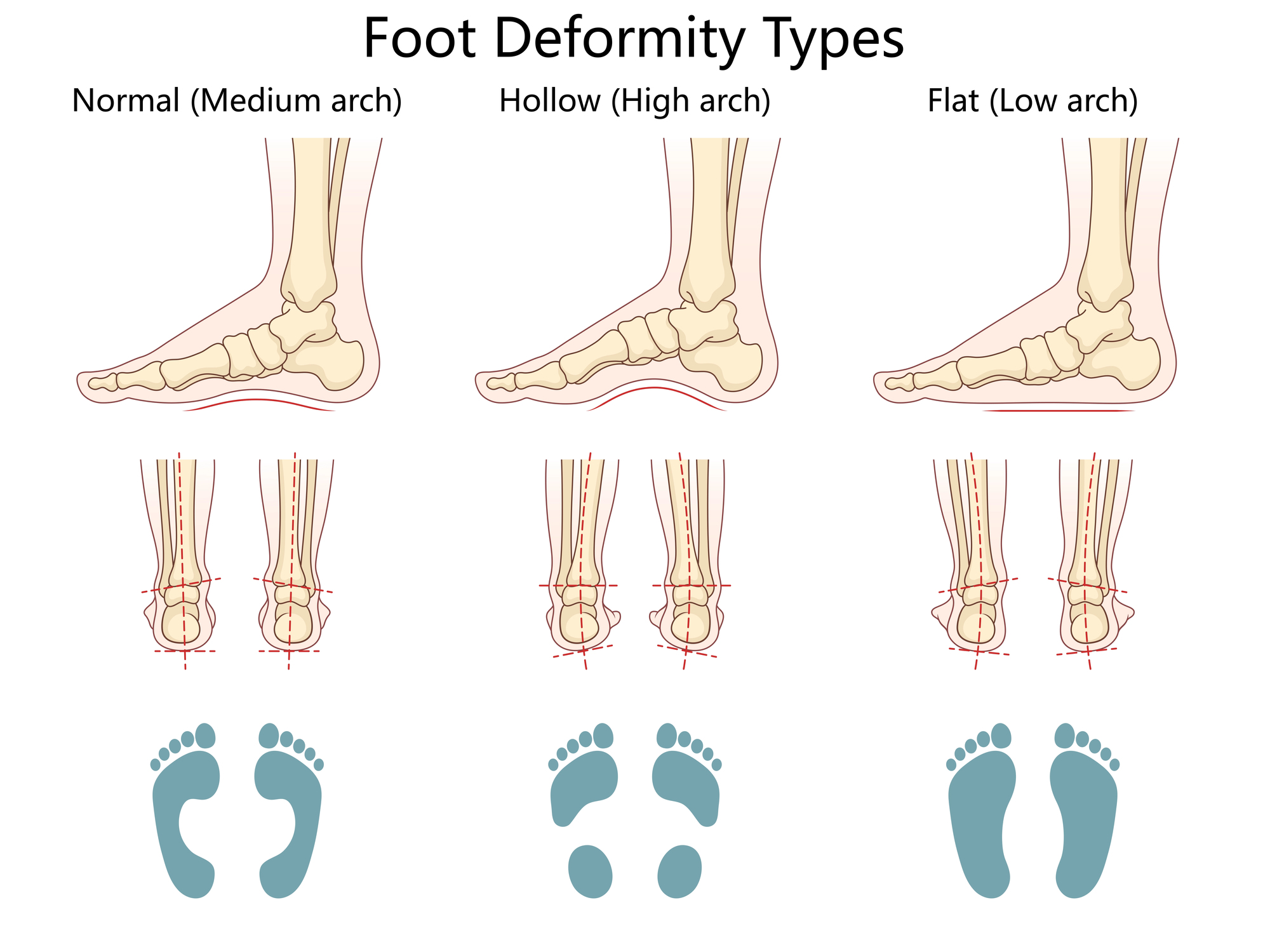
Flatfoot (pes planus) is the total or partial loss of the internal longitudinal arch of the foot, generally accompanied by an eversion of the rearfoot (calcaneal valgus) and, in many cases, by an abduction of the forefoot visible when observing the patient from behind (sign of “the many visible toes”). It is not a single disease: under this name coexist two clinically distinct entities that should be differentiated.
The flexible flatfoot is the most frequent. In children, it is physiological until the age of 5-6 years in most cases: the arch has not yet finished developing. It remains flexible in about 15-25% of healthy adults and, in itself, does not generate pathology if it is asymptomatic. When it hurts or limits activity, it deserves treatment.
Acquired adult flatfoot (AAPF) is a distinct entity: it appears between 40 and 60 years of age, almost always as a consequence of posterior tibial tendon dysfunction (PTTD). It is classified into four stages by Johnson and Strom according to evolution and stiffness. If detected early, it is perfectly controllable; if left untreated, it progresses to a rigid flatfoot with subtalar arthrosis that severely limits walking.
Symptoms: when does a flatfoot need treatment?
Asymptomatic flatfoot is not a disease. Flatfoot that is painful, fatiguing or has an impact on gait is. These are the signs that justify an evaluation in consultation:
- In the child: frequent falls, awkward gait, fatigue when walking for more than 30 minutes, asymmetrically worn shoes, spontaneous complaint of pain in the foot or calf at the end of the day.
- In young adults: diffuse pain in the inner aspect of the ankle and posterior tibial tendon area, discrete medial edema at the end of the day, calf cramps.
- In the middle-aged adult: progressive fall of the arch with age, pain in the medial aspect of the ankle (evolving PTTP), increasing difficulty to stand on tiptoe with only one foot.
- Sign of the “many visible toes”: when observing the patient from behind, 3 or more toes are seen protruding outside the heel (instead of one or two as in a normal foot).
- Pain in the sole of the foot, forefoot or heel due to compensatory overload.
- Pain radiating to the knee, hip or low back due to decompensation of the ascending kinetic chain.
- Asymmetrical shoe wear, especially at the inner edge of the heel.
- Sensation of “ankle going inward” in prolonged standing.
Why does flatfoot appear?
The causes of flatfoot are different depending on whether we are talking about children or adults. At Clínica San Román we clearly differentiate one from the other, because the effective treatment plan depends on identifying the real cause of the condition.
👶 Pediatric factors.
The arch of the foot is not fully formed at birth and develops with gait. Generalized ligamentous laxity (frequent, hereditary), childhood overweight, neuromuscular pathologies (cerebral palsy, muscular dystrophies) and, in rigid flatfeet, tarsal coalitions (anomalous bony joints between tarsal bones) are the protagonists. The vast majority are flexible, physiological and resolve on their own.
🦶 Posterior tibial dysfunction
It is the most common cause of adult acquired flatfoot. The posterior tibial tendon is the main dynamic stabilizer of the internal arch. Its weakness, chronic tendinopathy or rupture causes progressive arch drop, hindfoot valgus and forefoot abduction. It typically appears between 40 and 60 years of age, with a clear predilection for women, overweight, hypertension and diabetes. Without treatment, it progresses in stages.
⚖️ Overload and biomechanics
Overweight, prolonged standing on hard surfaces, flat shoes with little support and stiffness of the triceps suralis (shortening of the calf and soleus) overload the internal arch and accelerate its fall. Lower limb dysmetry, genu valgum and ankle equinus are frequent associated factors. Detecting and correcting the biomechanical substrate is key for the treatment to last.
Diagnosis: how do we evaluate flatfoot?
A good flatfoot diagnosis goes far beyond looking at the arch. Differentiating flexible/rigid, asymptomatic/symptomatic and functional stage of the posterior tibial tendon determines the treatment. At Clínica San Román we protocolize the evaluation in four levels:
🔍 Functional clinical examination
We assess the patient in standing, gait and dynamic tests. We apply the “single heel rise” test (ability to stand on tiptoe with only one foot, altered in TTPD), the sign of the many toes visible from posterior observation, flatfoot reducibility (flexible vs. rigid) in seated position and Jack’s maneuvers. This examination guides the diagnosis in most of the patients and allows to catalogue the functional stage.
📊 Computerized biomechanical study
Footprint analysis on prescanner and, where appropriate, force platform and video gait analysis. Objectively measures pressure distribution, degree of pronation, asymmetry between both feet and toe-off phase. Essential for designing effective insoles and for documenting progress before and after treatment.
📷 Bilateral loading radiography
Dorsoplantar projection, lateral in load and, depending on the case, axial projection of the calcaneus. It measures the Meary-Tomeno angle (axis of the talus-first metatarsal, altered in flatfoot), the Costa-Bertani angle, the angle of inclination of the calcaneus and signs of subtalar arthrosis. The radiograph in loading, not in unloading, is what provides real information.
🔊 Ultrasound and MRI of the posterior tibial.
In adult acquired flatfoot suspected of TTPD, dynamic ultrasound is used to assess continuity, thickness and peritendinous effusion of the posterior tibialis. MRI is the gold standard for staging tendinopathy or rupture, ruling out associated lesions of the spring ligament and planning surgery when appropriate.
Treatment of flatfoot: staging protocol by stage
The philosophy is minimal treatment is necessary depending on the stage. Most flatfeet can be controlled without surgery. When surgery is indicated, we always start with the least invasive option.
1 Conservative and biomechanical treatment
This is the basis. It combines custom insoles designed according to biomechanical study (with internal arch support, medial calcaneal post and, if appropriate, supinator rearfoot wedge), shoes with good containment and anatomical last, specific physiotherapy (posterior tibial strengthening with eccentric exercises, triceps suralis stretching, proprioception) and gait education. In stage I adult acquired flatfoot, this approach resolves or stabilizes a considerable majority of patients at 3-6 months. In the child, it slows progression when symptomatic.
2 Advanced orthosis and infiltration
When basic conservative treatment does not achieve the expected control after 3-6 months, we escalate to Arizona-type rigid orthoses (UCBL, semi-rigid wraparound support) in painful flexible stage II adult acquired flatfoot, and to ultrasound-guided infiltration of the posterior tibial tendon with PRP or selective corticosteroid when there is tendinopathy or frank tenosynovitis. These measures can maintain the patient without progression for years and, in many cases, avoid surgery.
3 Subtalar MIS subtalar arthroereisis
In symptomatic flexible flatfeet refractory to conservative treatment -both in selected pediatric patients (from sufficient bone maturity) and in adults in stage II-, minimally invasive subtalar arthroereisis is an effective alternative. It consists of the introduction of a small implant in the sinus of the tarsus (between the talus and the calcaneus) by means of a millimetric percutaneous incision, under local or regional anesthesia. It limits excessive pronation, restores the arch and normalizes mechanics. Immediate standing with walker boot, return to light activity 2-4 weeks and sport 10-14 weeks. The implant can be removed in the future if it loses indication.
4 Regulated reconstruction (advanced stages)
In stage III (rigid with incipient osteoarthritis) or IV (rigid with tibiotalar involvement) adult acquired flatfoot, the surgery becomes a planned reconstruction: medializing calcaneal osteotomy, flexor digitorum longus to posterior tibial transfer, lateral column lengthening and, in advanced cases, subtalar or selective triple arthrodesis. These procedures require outpatient or 24-hour admission, postoperative immobilization and prolonged rehabilitation. The indication and execution are coordinated with the referral orthopedic surgery and traumatology service.

Comparison of flatfoot treatments
| Criteria | Custom insoles | Arizona Orthosis + infiltration | MIS arthroereisis | Regulated reconstruction |
|---|---|---|---|---|
| Indication | Symptomatic, symptomatic flatfoot, children and adults stage I | Stage II flexible with DTTP, insole failure | Symptomatic refractory flexible (pediatric/adult) | Stage III-IV, stiff or with osteoarthritis |
| Invasiveness | Null | Minimal (puncture) | Percutaneous incision (mm), ambulatory | Open or combined surgery, inpatient |
| Recovery | Adaptation 1-2 weeks | No sick leave, spaced sessions | Immediate standing, sport 10-14 wk. | Immobilization 4-8 wks, rehab 4-6 months |
| Reversibility | Total | Total | Removable implant | Definitive |
| Evidence | Historical pillar, high adherence | Stabilization in stage II | Effective in refractory flexible foot | Gold standard in advanced stages |
Source: Johnson KA, Strom DE. Clin Orthop 1989; Bouchard M, Mosca VS. JAAOS 2014; Vora AM et al. JBJS 2006; Kohls-Gatzoulis J et al. BMJ 2009. Individual results may vary.
Advantages of MIS Flatfoot Surgery
You walk the same day
Immediate bipedestation with walker boot or post-surgical shoe, without plaster cast, without admission.
Local or regional anesthesia
No general anesthesia in most cases, no prolonged fasting, rapid recovery.
Millimeter incision
Almost imperceptible scar. Aesthetic result far superior to traditional open surgery.
Reversible if applicable
The arthroereisis implant can be removed in the future if it loses indication or discomfort appears.
Preserves future options
It does not burn bridges with major surgeries: if in the future there is a need for a regular reconstruction, it is still possible.
Objective restoration of the arch
Documented improvement in radiographic angles (Meary, Costa-Bertani) and postoperative prescan.
Maintenance and living with flatfoot
Controlled flatfoot requires maintenance to sustain the treatment outcome. These three levers summarize our discharge plan:
👟 Footwear and insole
Everyday shoe with good rearfoot containment, stable sole and wide last. Removable insole to use the customized one. Renewal of sports footwear every 600-800 km of use. Avoid long days with soft flatfoot shoes or flip-flops in patients with symptomatic flatfoot.
🦵 Strength and proprioception
Specific work on the posterior tibialis (guided eccentric exercises), strengthening of the intrinsic musculature of the foot (short foot exercise), daily stretching of the triceps suralis and balance work on unstable surfaces. Five to ten minutes a day makes a difference.
⚖️ Weight and periodic review
Body weight control: each extra kilogram increases the load on the arch. Podiatric check-up every 12-18 months in adults with symptomatic flatfoot and annually in pediatric patients until growth is consolidated. After surgery, scheduled check-ups at 3, 6 and 12 months, and then annually.

Do you suspect that you or your child has symptomatic flatfoot?
Differentiating physiological from pathological is what separates a simple follow-up from a treatment that avoids future problems. We study the footprint, assess the posterior tibial tendon and design a plan adapted to the stage.
Request your free evaluationFrequently Asked Questions about flatfoot
We solve the most common doubts of our patients and their families.
👶 Child’s flatfoot
Is the child’s flatfoot operated on?
Almost never. Flatfoot in children up to 5-6 years of age is physiological in the vast majority of cases and resolves spontaneously with arch development. The usual approach is observation, appropriate footwear and, if there is pain or functional limitation, custom insoles. Pediatric surgery is reserved for rigid flatfeet with bony bar (synostosis), symptomatic flatfeet refractory after bony maturity or with neurological etiology.
Does my child need insoles if he/she has flatfeet?
Not systematically. Until the age of 5-6 years the arch is forming and most children have physiological flatfoot that does not require treatment. We indicate insoles when there is pain, fatigue when walking, frequent falls, marked asymmetry between both feet or when the flatfoot is associated with overweight, generalized laxity or neurological disorders. A podiatric assessment between 4 and 7 years of age allows us to differentiate between physiological and pathological conditions.
At what age do you have surgery if you do not improve?
The vast majority of pediatric flatfeet do not require surgery. If symptomatic persists after exhausting conservative treatment and there is an indication, minimally invasive subtalar arthroereisis is typically performed from the age of 9-12 years, when the foot has matured sufficiently. Each case is evaluated on an individual basis: age, weight, symptoms, bone structure, neurological substrate and response to previous treatment.
🦶 Adult Flatfoot
What about adult flatfoot?
Adult acquired flatfoot (AAPF) is a distinct entity from infantile flatfoot. In most cases it is secondary to posterior tibial tendon dysfunction (PTTD), appears between 40 and 60 years of age, with a clear predilection for women, and is classified into four stages by Johnson and Strom according to evolution and stiffness. Its treatment is stage-dependent.
What is subtalar arthroereisis?
It is a minimally invasive surgical technique in which a small implant is inserted in the sinus of the tarsus, between the talus and the calcaneus, to limit excessive pronation of the subtalar joint and restore the arch. It is performed by a few millimeters incision, under local or regional anesthesia, on an outpatient basis. It is a reasonable alternative in symptomatic flexible flatfeet – both pediatric and adult stage II – refractory to conservative treatment.
Can it get worse if left untreated?
The flexible flatfoot of the child rarely progresses. Adult acquired flatfoot does: untreated posterior tibial tendon dysfunction progresses from a painful flexible flatfoot (stage I-II) to a rigid flatfoot with subtalar and midtarsal arthrosis (stage III-IV), which already requires major reconstructive surgery. Early detection and treatment of stage I-II prevents progression in many cases.
How does it relate to knee, hip or back pain?
Flatfoot alters the ascending kinetic chain. Excessive pronation of the rearfoot causes internal rotation of the tibia, which drags the femur and modifies the mechanics of the knee, hip and pelvis. In clinical practice we see decompensated flatfeet associated with anterior knee pain, patellar or Achilles tendinopathy, external hip pain and low back overload. Therefore, the approach always includes a global postural assessment.
🏥 Treatment
Do insoles cure flatfoot?
No, but they control it. A well-designed custom insole reduces posterior tibial tendon overload, improves pressure distribution, relieves pain and slows down the progression of the condition in a considerable majority of patients. In children’s flatfoot it facilitates walking and reduces fatigue; in adults it prevents or delays surgery. It does not correct bone structure, but stabilizes function.
How long does recovery take after MIS arthroereisis?
After minimally invasive subtalar arthroereisis, most patients walk from the same day with a walker boot or post-surgical shoe. We reintroduce normal footwear with insole at 2-3 weeks, light activity at 4-6 weeks and impact sport at 10-14 weeks, with intermediate clinical assessment. Time frames vary according to age and sporting profile.
Is it surgery with plaster cast and long discharge?
It depends on the technique. MIS arthroereisis allows walking with a walker boot or post-surgical shoe from the same day, without plaster, with return to work in 2-4 weeks in sedentary jobs. More complex surgical reconstructions (calcaneal osteotomies, tendon transfers, selective arthrodesis) do require a longer period of immobilization and rehabilitation.
I am older: am I in time for surgery?
Yes, as long as the indication is correct and the general condition allows it. Age alone is not a contraindication. What changes is the strategy: older patients with rigid flatfoot and osteoarthritis often benefit more from selective arthrodesis type solutions than from long tendon reconstructions. MIS surgery, when indicated, maintains the advantages of short operative time and rapid standing.
Scientific references
- Johnson KA, Strom DE. Tibialis posterior tendon dysfunction. Clin Orthop Relat Res. 1989;239:196-206.
- Kohls-Gatzoulis J, Angel JC, Singh D, et al. Tibialis posterior dysfunction: a common and treatable cause of adult acquired flatfoot. BMJ. 2004;329(7478):1328-1333.
- Bouchard M, Mosca VS. Flatfoot deformity in children and adolescents: surgical indications and management. J Am Acad Orthop Surg. 2014;22(10):623-632.
- Vora AM, Tien TR, Parks BG, et al. Correction of moderate and severe acquired flexible flatfoot. J Bone Joint Surg Am. 2006;88(8):1726-1734.
- Bowring B, Chockalingam N. Conservative treatment of tibialis posterior tendon dysfunction: a review. Foot. 2010;20(1):18-26.
- Mosca VS. Flexible flatfoot in children and adolescents. J Child Orthop. 2010;4(2):107-121.
- Henderson AA, Hawes MR. The pediatric flat foot. Phys Med Rehabil Clin N Am. 2014.
Information prepared by the medical team of Clínica San Román. Center No. 5357 Autonomous Registry of Health Centers, Services and Establishments of the Valencian Community. This page is for information purposes only and does not replace the individual clinical assessment.
Take care of your arch from the foot
Biomechanical diagnosis, custom insoles, MIS surgery when appropriate. We have been treating children and adult flatfeet in Alicante since 1979.
- 📞 +34 965 921 156
- ✉️ info@clinicasanroman.com
- Av. del Dr. Ramón y Cajal 1, 03001 Alicante