
SPORTS PODIATRY – TARSAL SINUS SYNDROME – ALICANTE
Tarsal sinus syndrome treatment: we stabilize your ankle and get you back to work.
Stabilizing insoles + proprioception – Ultrasound-guided infiltration when there is synovitis – MIS arthroscopy if the condition is chronic – 45 years treating athletes in Alicante.

Backed by 45 years of experience
Clinic founded in 1979
Four and a half decades treating ankle instabilities and sports foot pathologies in Alicante.
Certification MIS23BE03 ABMSP
European pioneers in minimally invasive surgery of the foot accredited by the American Board of Multispecialty Surgical Podiatry.
Multilingual service
We attend you in Spanish, English, German, French and Dutch.
What is tarsal sinus syndrome?
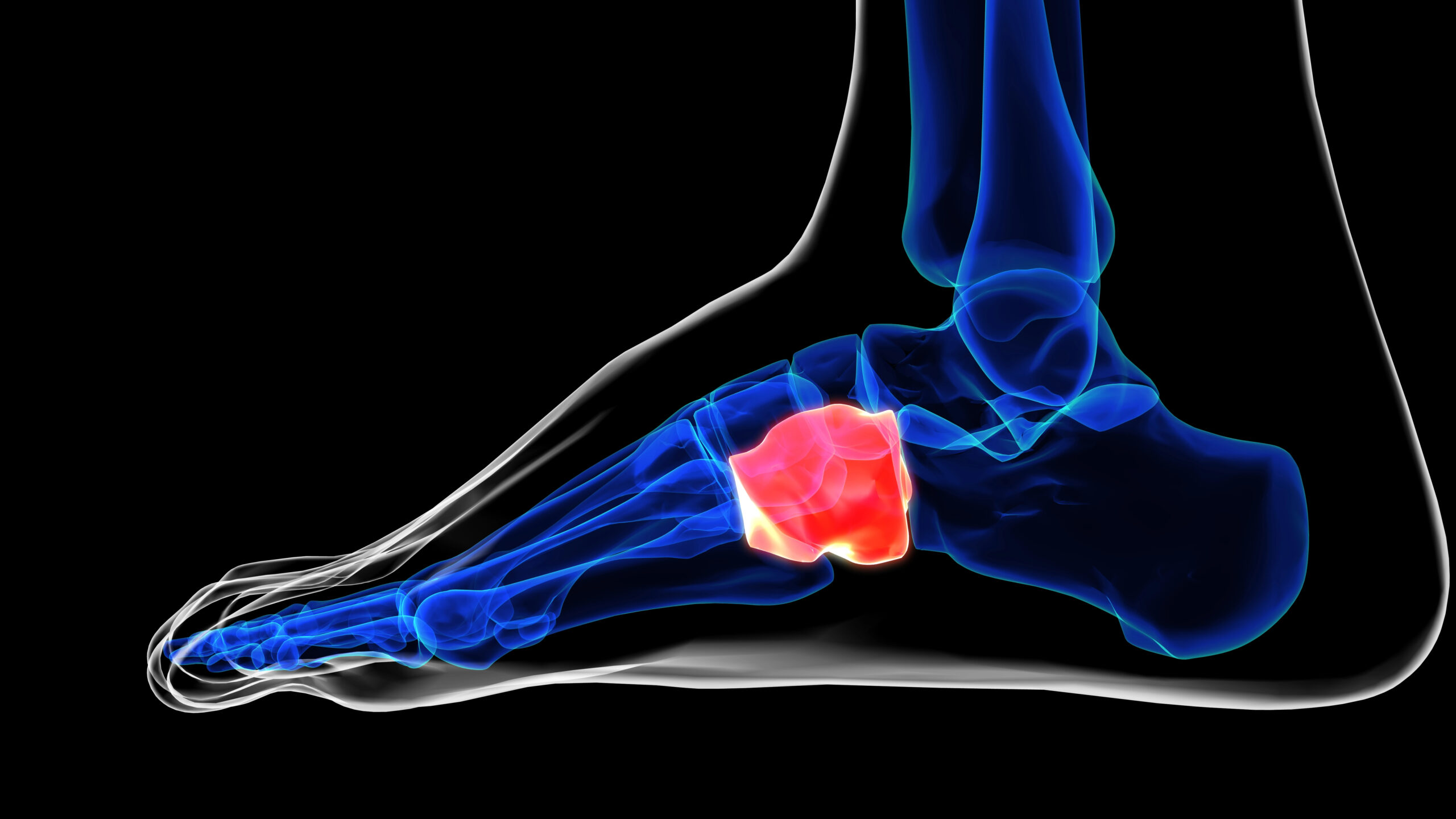
The sinus tarsi is a small cone-shaped anatomical space located between the talus (above) and the calcaneus (below), open towards the external aspect of the foot just in front of the lateral malleolus. Inside it houses the astragalocalcaneal interosseous ligament, proprioceptive nerve branches, vessels and synovial tissue. It is, in a sense, the “control center” of the subtalar joint and plays a key role in ankle stability and sensory information.
Tarsal sinus syndrome is the clinical picture that appears when this space becomes inflamed or unstable: pain on the external aspect of the ankle, persistent sensation of “my foot is slipping” and difficulty on uneven ground. The most frequent cause, described in the literature since the 1950s, is repetitive inversion sprains: after a poorly rehabilitated sprain, the capsule and the interosseous ligament become chronic as post-traumatic synovitis (Klausner VB & Hardy MA, 1997).
Several studies point out that this is an underdiagnosed cause of chronic ankle pain in athletes, especially runners, paddle tennis players, soccer players, basketball players and dancers, and that confirmation with MRI is key because plain radiography is usually normal (Lektrakul N, et al. 2001).
Symptoms: How to recognize tarsal sinus syndrome?
The classic picture is a selective pain in the external aspect of the ankle, just in the dimple that is noticed in front of the malleolus, accompanied by an uncomfortable sensation of “loose ankle” or “insecure”. It usually appears weeks or months after a sprain and, what exasperates the patient the most, it does not go away with rest. It worsens when walking on uneven ground, when changing direction or when starting to walk in the morning.
- Pain in the external aspect of the ankle and tarsal sinus, reproducible on palpation.
- Feeling of instability (“my foot goes”), especially on uneven surfaces or when turning.
- History of one or more previous inversion sprains.
- Pain when starting to walk after sitting or in the morning when getting up.
- Worsening with sports activity, especially running, paddle tennis and change of direction sports.
- Tightness when stepping on a curb or uneven ground.
- Partial improvement with rest, recurrence on return to activity.
- Intermittent swelling in the external area of the ankle after exertion.
Why does tarsal sinus syndrome appear?
In the vast majority of cases there is a traumatic antecedent: a sprain -or several- that did not heal well. Subsequent instability and synovitis of the tarsal sinus are the two ways in which the condition becomes chronic. These are the three mechanisms that we see most frequently in consultation.
⚽ Repetitive sprains
Acute inversion sprain is probably the most common musculoskeletal injury. When repeated or poorly rehabilitated, the anterior peroneo-talar, peroneo-calcaneal and sinus interosseous ligaments become lax and the subtalar joint loses stability. This secondary laxity maintains constant microirritation of the tarsal sinus and triggers the syndrome.
🦶 Chronic subtalar instability
The subtalar joint (between the talus and the calcaneus) is responsible for adapting the foot to the ground. If it loses control – due to ligamentous laxity, proprioceptive deficit or hyperpronator gait – the tarsal sinus is subjected to abnormal mechanical stress. Helgeson (2009) describes how proprioceptive deficit is one of the key factors that maintain the condition in athletes.
🩹 Post-traumatic sinus synovitis.
After the initial trauma, the synovial tissue lining the sinus becomes inflamed, proliferates and produces a true chronic “bursitis” that perpetuates the pain even when mechanical instability is already mild. It is the lesion best visualized by magnetic resonance imaging and the one that most benefits from ultrasound-guided infiltration or, in refractory forms, from arthroscopic cleaning.
Diagnosis: how do we confirm tarsal sinus syndrome?
The diagnosis is clinical-radiological and, when there are doubts, it is closed with an anesthetic block of the sinus: if the injection of lidocaine takes away the pain for a few hours, the test is practically confirmatory.
🔍 Clinical examination + inversion test
We collect the sprain history, assess the static and dynamic gait, check lateral stability and reproduce the pain with selective palpation of the sinus and with the forced inversion-supination test. A palpation that exactly reproduces “your” pain in the lateral dimple is a very powerful clue.
🔊 Ultrasound and magnetic resonance imaging
Plain radiography is usually normal and only rules out other pathologies (tarsal coalition, small fractures). Magnetic resonance imaging is the gold standard: it shows the edema of the interosseous ligament, sinus synovitis and possible hidden associated lesions (Lektrakul N, et al. 2001). Ultrasonography is also useful to assess the state of the peroneals and to guide the infiltration.
💉 Diagnostic-therapeutic blockade
When all of the above is suggestive but not conclusive, we infiltrate the tarsal sinus with local anesthetic guided by ultrasound. If the pain disappears during the following hours, we confirm the origin of the condition and orient the treatment. This is the most specific test available for this pathology and, in addition, it usually has a therapeutic effect that lasts for days or weeks.
Treatment of tarsal sinus syndrome: stepwise protocol.
Our philosophy is “less is more”. In the tarsal sinus, moreover, conservative treatment works very well in the majority of patients: it is one of the conditions where the combination of insoles, proprioception and muscle reinforcement has the greatest chance of success before any surgery is considered. Arthroscopic surgery is reserved for refractory cases.

1 – Conservative treatment: insoles + proprioception
Tailored stabilizing insoles with external wedge to control subtalar instability and unload the sinus, progressive proprioception program (monopodal support, unstable platform, sport gestures), selective peroneal and tibialis posterior reinforcement, physiotherapy with hindfoot mobilization techniques and, if necessary, functional protective taping during return to activity. Helgeson (2009) describes very favorable responses with this approach in properly selected athletes.
2 – Ultrasound-guided infiltration of the breast
When there is synovitis demonstrated by MRI or ultrasound and the initial conservative treatment does not control the condition, we infiltrate the sinus under ultrasound control. We use corticoid in “pure” inflammatory forms, platelet-rich plasma (PRP) in sports patients seeking tissue regeneration or hyaluronic acid when the subtalar component is predominant. We individualize the regimen and product according to the patient’s profile and the stage of the condition.
3 – Arthroscopic sinus surgery (cleaning)
Reserved for cases in which the synovitis is chronic and does not respond to several months of conservative + well indicated infiltrations. By means of minimally invasive arthroscopy we introduce a few millimeters optic and clean the inflamed synovial tissue of the sinus, also evaluating the interosseous ligament and other associated lesions. No plaster cast, no screws, same-day discharge and a clearly faster return to sports than with open surgery.
Tarsal sinus syndrome treatment comparison
| Criteria | Insoles + proprioception | Ultrasound-guided infiltration | MIS arthroscopy | Traditional open surgery |
|---|---|---|---|---|
| Indication | Mild-moderate instability, first approach | Demonstrated synovitis, failure of step 1 | Refractory chronic synovitis, associated lesions | Complex instabilities, extensive ligamentous reconstructions |
| Invasiveness | Null | Minimal (needle, echo) | Minimal (millimeter portals) | High (wide incision, open dissection) |
| Anesthesia | No infiltrative | Local infiltrative | Regional or local + sedation | Spinal or general |
| Sessions / time | 8-12 week program | 1-3 infiltrations every 4-6 weeks | Single outpatient procedure, ~30-45 min | Hospitalization, cast 2-4 weeks |
| Expected efficacy | Good in most non-chronic cases (Helgeson 2009) | Significant relief in the short-medium term | High in chronic synovitis | High, with higher morbidity and longer sports leave |
Why choose Clínica San Román
🏃 Experience with sports patients
Runners, paddle tennis players, basketball players, soccer players, dancers: we have been treating athletes of all levels in Alicante for 45 years.
🧠 Conservative approach first.
The tarsal sinus responds very well to templating and proprioception. We only scale if the case does not respond – we do not operate by system.
🩺 Ultrasound-guided infiltration in the office
We perform the infiltrations under ultrasound control in our own office: maximum precision and better safety.
✂️ MIS Arthroscopy if needed
When it is necessary to enter the sinus, we do it with millimetric portals. No plaster, no screws, same day discharge.
📊 Complete biomechanical study
Pressure platform, gait video and footprint analysis: we measure to adjust the insole with precision.
🤝 Coordination with your physio or physician.
We work in a network with physiotherapists, traumatologists and physical trainers. If you already have a team, we join the plan.
Prevention of tarsal sinus syndrome
The best prevention is the correct rehabilitation of the initial sprain. If you have already had one or more, there are three pillars to prevent it from becoming chronic in the tarsal sinus.
👟 Stabilizing shoes and inserts
For sports: a shoe with a good counter, a sole with lateral support and a stable last. For daily life: avoid a flat shoe with a soft, uneven sole. If your rearfoot is unstable, a custom-made stabilizing insole makes a difference.
🤸 Sustained proprioception
Monopodal support with eyes closed, bosu, unstable plate, controlled jumps, reactive exercises. It is enough 10-15 minutes several times a week to maintain the “memory” of the ankle and prevent new sprains.
💪 Peroneal strengthening
The peroneals are the muscles that prevent the ankle from “falling” inward. Working them with elastic bands, eccentric exercises and progressive resistance is the best active protection against sprains and, by extension, against tarsal sinus syndrome.

Do you still notice instability months after a sprain?
The problem may be in the sinus of the tarsus. We evaluate you without obligation, do a gait analysis and explain what we can do in your case.
Request your free evaluationFrequently asked questions about tarsal sinus syndrome
We solve the most common doubts of our patients.
🔬 About the pathology.
What exactly is the tarsal sinus?
It is a small cone-shaped anatomical space located between the talus and the calcaneus, open towards the external aspect of the foot in front of the lateral malleolus. Inside there is an interosseous ligament, proprioceptive nerve branches and synovial tissue. It is one of the regulators of rearfoot stability and, when it becomes inflamed or unstable after sprains, the clinical picture discussed on this page appears.
How is it different from a chronic sprain?
The acute sprain affects mainly the anterior peroneo-talar ligament; the tarsal sinus syndrome is the late consequence: pain in the external aspect, sensation of instability and synovitis inside the sinus. Many times both pictures coexist: there is lateral laxity plus internal synovitis of the sinus. Magnetic resonance imaging is the test that best differentiates them and guides the treatment (Lektrakul N, et al. 2001).
Can I continue running with this injury?
It depends on the phase. In mild cases, well controlled with insoles, proprioception and functional bandaging, many patients maintain a reduced activity without worsening. In acute phases with frank synovitis and daily pain, it is advisable to reduce volume and intensity or rest for a few weeks to avoid chronification of the injury. The rule of thumb: if pain limits you, listen to your foot and be guided by the assessment.
Are the templates sufficient?
In a significant proportion of patients, yes. Custom-made stabilizing insoles, combined with a proprioception and peroneal strengthening program, control the instability and allow the synovitis to subside. If you have had the condition for a long time or the MRI shows very established synovitis, it is likely that insoles alone will not be sufficient and will have to be combined with infiltration or arthroscopy.
🏥 Treatment
What does breast infiltration consist of?
The medication (corticosteroid, platelet-rich plasma or hyaluronic acid) is injected directly into the sinus of the tarsus under ultrasound guidance. The needle enters the external aspect of the ankle guided in real time to deposit the product in the exact site. It is ambulatory, lasts a few minutes and, in many patients, it also serves as a diagnostic test: if the pain disappears after the infiltration, we confirm the origin of the condition.
What percentage of patients improve without surgery?
The available literature is heterogeneous, but agrees that a majority of patients with tarsal sinus syndrome respond to well-designed conservative treatment (insoles + proprioception ± infiltration). Helgeson (2009) and other authors describe favorable responses avoiding surgery in a notable proportion of cases. Arthroscopic surgery is reserved for patients who do not respond after several months of correctly applied conservative treatment.
Does arthroscopy leave sequelae?
Tarsal sinus arthroscopy is performed through millimetric portals, so scars are practically imperceptible and the risk of adhesions or stiffness is low compared to open surgery. Like any intervention, it is not free of risks (infection, nerve injury of sensitive branches, residual pain), but in trained hands they are rare. We detail risks and expectations in the preoperative consultation.
🏃 Recovery and prevention
How long does it take me to return to training after an infiltration?
With corticosteroid, we recommend 48-72 hours of very reduced activity and progressive reincorporation to training during the first week. With PRP, the protocol is somewhat more conservative: 7-10 days of reduced load and 3-6 weeks to return to previous performance, depending on the sport. The idea is not to “cover” the pain with the infiltration and return to the injury stimulus immediately: the improvement that the infiltration provides must be used to rehabilitate.
Can it be prevented after a sprain?
Yes, the most effective measure is the correct and complete rehabilitation of the initial sprain: 4-6 weeks of guided proprioception, peroneal strengthening and progressive return to sport. A stabilizing insole during the first months post-sprain and a functional bandage on return to practice add security. Most of the tarsal sinus syndromes that we see in consultation come from sprains treated only with rest and anti-inflammatory medication, without specific rehabilitation.
Scientific references
- Helgeson K. Examination and intervention for sinus tarsi syndrome. N Am J Sports Phys Ther. 2009;4(1):29-37. [PMID: 21509110]
- Klausner VB, Hardy MA. Sinus tarsi syndrome: a clinical entity with somatosensory evoked potential. J Foot Ankle Surg. 1997;36(2):133-7. [PMID: 9127227].
- Lektrakul N, Chung CB, Lai YM, Theodorou DJ, Yu J, Haghighi P, Trudell D, Resnick D. Tarsal sinus: arthrographic, MR imaging, MR arthrographic, and pathologic findings in cadavers and retrospective study data in patients with sinus tarsi syndrome. Radiology. 2001;219(3):802-10. [PMID: 11376274]
- Pisani G, Pisani PC, Parino E. Sinus tarsi syndrome and subtalar joint instability. Clin Podiatr Med Surg. 2005;22(1):63-77. [PMID: 15555844]
- Akiyama K, Takakura Y, Tomita Y, Sugimoto K, Tanaka Y, Tamai S. Neurohistology of the sinus tarsi and sinus tarsi syndrome. J Orthop Sci. 1999;4(4):299-303. [PMID: 10436277]
- Oloff LM, Schulhofer SD, Bocko AP. Subtalar joint arthroscopy for sinus tarsi syndrome: a review of 29 cases. J Foot Ankle Surg. 2001;40(3):152-7. [PMID: 11417596]
This page is for information purposes only and does not replace the individual clinical assessment. Each case requires a personalized examination.
Don’t let an unstable ankle control your sport and your day-to-day life.
If you have been suffering for months from pain on the outside of your ankle after a sprain, we can help you. We will assess you, do a biomechanical study and propose a plan tailored to your needs – no pressure and no empty promises.
- 📞 +34 965 921 156
- ✉️ info@clinicasanroman.com
- Av. del Dr. Ramón y Cajal 1, 03001 Alicante