
PODIATRY BIOMECHANICS – KNEE PAIN – ALICANTE
Knee pain treatment: when the cause starts in the foot
Biomechanical study of the footprint – Custom insoles – Corrective MIS foot surgery when the deformity drags to the knee.

Backed by 45 years of experience
Clinic founded in 1979
Three generations of podiatrists specialized in lower limb biomechanics and MIS foot surgery in the center of Alicante.
Certification MIS23BE03 – ABMSP
European pioneers certified by the American Board of Multispecialty in Podiatry in minimally invasive surgery of the foot.
Multilingual service
We attend you in Spanish, English, German, French and Dutch. Center nº 5357 of the Health Registry of the Valencian Community.
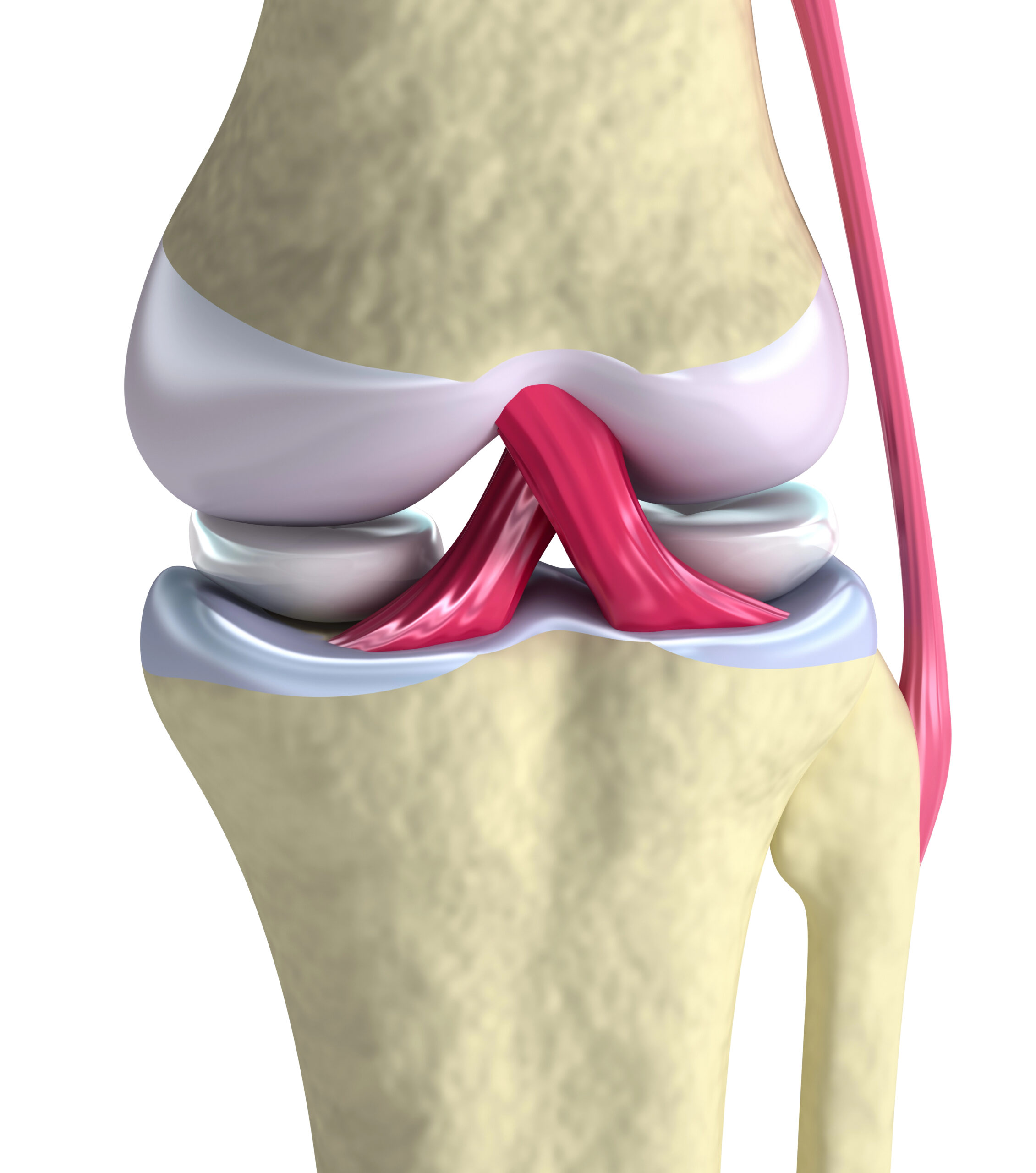
What is biomechanical knee pain?
Knee pain of biomechanical origin is that which does not originate in the joint itself, but is transmitted from an altered plantar support. The knee is an intermediate joint: it receives everything that comes from below (foot, ankle) and everything that comes from above (hip, pelvis). When the foot is incorrect -pronator, supinator or asymmetric- the load axis of the knee is displaced a few degrees, and this small deviation, repeated thousands of times a day, ends up producing anterior, lateral or retropatellar pain.
In clinical terms we speak of pain secondary to an alteration of the lower kinetic chain. The knee is not the culprit: it is the victim of what happens on the ground. That is why the approach from biomechanical podiatry is key when the orthopedic surgeon has ruled out meniscal, ligament or advanced degenerative injury and, nevertheless, the pain persists. Several studies indicate that between 20% and 30% of chronic gonalgias improve significantly by correcting plantar support (Barton et al., JOSPT 2010; Collins et al., consensus 2018).
At Clínica San Román we do not operate on the knee: we complement the work of your orthopedic surgeon and your physiotherapist by detecting if there is a component of the foot that is adding load to the joint. If there is, we treat it; if there is not, we tell you honestly and refer you.
Symptoms: how to recognize podiatric knee pain?
Knee pain with a biomechanical component usually has a very characteristic pattern: it appears or worsens with weight-bearing activity, improves with rest and reappears when walking again. It is not always associated with a specific trauma; often the patient tells us that “it started gradually, without knowing why”. These are the symptoms we see most often in consultation:
- Anterior knee pain (around or behind the kneecap), especially when going up or down stairs.
- Lateral or medial pain when walking long distances or running.
- Sensation of instability or “failure” of the knee on uneven terrain.
- Crepitus (audible clicks) on flexion and extension, without joint locking.
- Pain that appears after standing for a long time, even without walking.
- Increased pain at the end of the day or after a day of standing work.
- Asymmetry: one knee hurts more than the other (usually coincides with the side of the more pronated foot or longer leg).
- Pain that improves with absolute rest and reappears at the first walk.
Why does knee pain occur from the foot?
The knee is trapped between two very mobile joints -the ankle below and the hip above-. Any misalignment at these extremes ends up calling the knee to account, which has limited mobility to compensate. At Clínica San Román we group the most frequent biomechanical causes into three blocks:
🦶 Pronator or supinator stride
Excessive pronation depresses the internal arch and rotates the tibia inward: the patella is decentered and anterior pain appears. Supination, on the contrary, transfers all the load to the external border and overloads the lateral compartment. Both patterns, maintained over time, are responsible for patellofemoral syndrome and iliotibial band syndrome, two of the most frequent causes of gonalgia in runners and habitual walkers.
⚖️ Lower limb dysmetry
A leg length difference greater than 5-8 mm systematically overloads the knee on the longer side, which has to “hold” the body weight longer with each step. Dysmetry can be anatomical (the bone is shorter) or functional (due to pelvic tilt, contractures, etc.). Detecting it and compensating for it with an insole radically changes the distribution of loads on the hip, knee and lumbar spine.
👣 Forefoot pathology that impairs gait
A painful bunion, hallux rigidus or claw toes cause the patient to unconsciously modify his or her gait so as not to support the painful area. This antalgic gait shifts the load to the outer edge of the foot and forces a rotation of the knee which, in a few months, translates into joint pain. Treating the forefoot – conservatively or with MIS surgery – is often the missing piece of the puzzle.
Diagnosis: how we confirm the biomechanical origin of your knee pain
Confirming that the foot is the real cause of knee pain requires measuring, not guessing. In the first consultation we combine manual examination, gait observation and gait analysis technology to build an objective, reproducible diagnosis that can be shared with your orthopedic surgeon or physiotherapist.
🔍 Clinical examination and observation of gait.
We start with a detailed clinical history, palpation of the painful points in the knee and specific tests (patellar compression, Ober maneuver, assessment of the varus/valgus axis). We then ask you to walk barefoot and in shoes to observe stance, toe-off and swing phases. Step asymmetry, tibial internal rotation or arch collapse are immediate clues that guide the rest of the study.
📊 Biomechanical study of the footprint.
We carried out the study on a static and dynamic pressure platform. We measured how the weight is distributed between both feet, the trajectory of the center of pressures and the contact times. We analyze the rearfoot angle, knee valgus and hip tilt on a tape with camera. The result is an objective report with numerical values that allow comparison before and after treatment.
📷 Supplementary image
When appropriate, we complete with a loaded foot X-ray to confirm structural deformities (bunion, hallux rigidus, Lisfranc subsidence) and to rule out established joint pathology. If your traumatologist has not requested it, we also ask for pelvis and knee X-rays in load to rule out anatomical dysmetry. MRI is reserved for specific cases and always referred.
Biomechanical knee pain treatment: stepwise protocol.
Our philosophy is “less is more”: we always start with the least invasive option that provides the best result. MIS foot surgery is only considered when there is a clear structural deformity that is altering gait. Most patients with biomechanical knee pain improve in steps 1 and 2.
1 Custom insoles with gait analysis
The first step is always the custom insole, made from the 3D mold of your foot and the pressure platform report. It is not a generic pharmacy insole: it corrects the exact degree of pronation/supination, compensates for the millimeters of dysmetry detected and relieves the areas of hyperpressure. We manufacture it in thermoformable materials for prolonged use and we check it after 4-6 weeks to adjust what the body tells us. We always accompany with footwear guidelines and, if overweight, with a realistic handling advice.
2 Gait reeducation and advanced therapies
When the insole provides improvement but is not sufficient, we add gait pattern re-education (hip, gluteus medius and conscious gait work) in coordination with your physiotherapist. If the examination detects a secondary enthesopathy in the patellar tendon or goose foot, we apply shock waves (ESWT) in the area. Scientific evidence supports this combination in patellofemoral syndrome and chronic tendinopathies (Mills K et al., 2012).
3 MIS corrective foot surgery
Only when the origin of the knee pain is a structural foot deformity (severe bunion, advanced hallux rigidus, fixed claw toes) that demonstrably alters gait. Minimally invasive surgery (MIS) is performed with local anesthesia, millimeter incisions and no screws in most cases. You walk the same day with a post-surgical shoe. Important: this surgery corrects the foot, not the knee. The improvement of the knee comes as a result of returning a physiological gait.

Comparison of options for biomechanical knee pain
| Criteria | Custom template | Generic insole | MIS foot surgery | Conservative management only (no foot) |
|---|---|---|---|---|
| Indication | Pain with objective alteration of the footprint. | Mild discomfort without previous study | Structural deformity of the forefoot | Pure joint injury without podal component |
| Invasiveness | Null (external device) | Null | Minimal (millimeter incisions) | Null |
| Anesthesia | No anesthesia required | Not required | Local | Not required |
| Time to improvement | 2-8 weeks | Variable, no guarantee | 3-6 months postoperative | Variable according to pathology |
| Documented efficacy | Improvement of pain in 60-75% of gonalgias with biomechanical component (Barton et al., JOSPT 2010; Collins et al., consensus 2018) | Limited and not individualized | High on deformity; knee improvement due to secondary effect. | Effective when there is no foot component |
Source: Barton CJ et al. JOSPT 2010; Mills K et al. Br J Sports Med 2012; Collins NJ et al. Br J Sports Med 2018 (consensus). Individual results may vary.
Why choose Clínica San Román for your knee pain?
45 years of family experience
Three generations of podiatrists specializing in lower limb biomechanics and MIS foot surgery.
Biomechanical study with technology
Pressure platform, dynamic gait analysis and loading X-ray. We measure before treating.
Conservative approach first
We always start with templating and reeducation. We only perform surgery if the structure requires it.
MIS surgery if necessary
European pioneers in MIS of the foot. Local anesthesia, millimetric incision, immediate ambulation.
Coordinated multidisciplinary team
We work in network with traumatologists, rheumatologists and physiotherapists in Alicante. We share report.
Objectively measurable improvement
We compare pressure platform before and after. If there is no change, we say so. No blind loyalty.
Prevention of knee pain from the foot
👟 Footwear suitable for your activity
Renew your running shoes every 600-800 km of use. Avoid shoes with excessive drop or completely flat soles if you have not worked on them. For daily use, look for a wide forefoot last, a firm heel counter and a supportive closure. A shoe that “shows” is a poorly chosen shoe.
🏃 Gluteus medius and core strengthening
Gluteus medius weakness is the silent cause of many knee pains. Work weekly side bridges, one-legged squats and elastic band in abduction. Five minutes a day of core stabilizes the entire chain. Your knee will not suffer if the hip works.
⚖️ Weight management and progressive loading
Every extra kilo multiplies by 4 times the load on the knee when climbing stairs. No need for obsessive scales: sustainable habits are enough. And if you resume running after a break, increase your volume by 10% per week, no more. The knee is not forgiving of rushing.

Does your knee hurt but they tell you your feet are fine?
The chain starts at the bottom. If you have been in pain for months and no one has looked at your dynamic footprint, we invite you to a free evaluation. We study, measure and explain what we have found, honestly and without obligation.
Request your free evaluationFrequently asked questions about knee pain
We solve the most common doubts of our patients.
🔬 About the pathology.
Can my foot be the real cause of my knee pain?
Yes, and it is more common than it seems. The knee is trapped between the ankle and hip, and absorbs the misalignments of both. A pronated stride rotates the tibia inward, off-centers the patella and produces anterior pain; a dysmetry of a few millimeters overloads the knee on the longer side. Several studies indicate that between 20 and 30% of chronic gonalgias improve when the plantar support is corrected.
What is a biomechanical gait analysis and what does it include?
It is an objective analysis of how you support the foot in static and walking. It includes medical history, manual examination, pressure platform, tape recording with camera and, when appropriate, loaded foot X-ray. The test lasts between 45 and 60 minutes and we provide a report with comparable numerical values before and after treatment.
How is a bunion related to knee pain?
A painful bunion unconsciously modifies the way you walk: you shift your weight to the outer edge of the foot so as not to support the bunion area. This antalgic gait forces a rotation of the tibia and a dynamic knee valgus that, maintained for months or years, produces joint pain. Treating the bunion restores the gait pattern and, in many patients, relieves knee pain as a result.
Is this treatment covered by insurance?
The biomechanical study and custom-made insoles are considered podiatric treatment. Some private insurances cover the consultation or a percentage of the insoles; it is advisable to check with your mutual insurance company. MIS foot surgery is usually covered by most insurers when there is a documented clinical indication.
🏥 Treatment
Are the templates forever?
Not necessarily. Insoles last on average 18-24 months depending on use and impact, and should be checked annually. In some functional footsteps they can be removed after months of improvement if you have worked on strengthening. In structural footsteps the insole accompanies continuously.
Do I have to have foot surgery if my knee hurts?
Almost never. MIS foot surgery is only considered when there is a clear structural deformity (severe bunion, hallux rigidus, fixed claw toes) that demonstrably alters gait and does not respond to conservative treatment. The vast majority of patients with biomechanical knee pain improve with custom insoles and re-education.
How much time do I need to notice improvement with insoles?
The first few days your body adapts to the new insole and you may notice slight arch or calf discomfort; this is normal. The improvement of knee pain usually starts to be noticed between the second and fourth week, and consolidates around 6-8 weeks.
🏃 Recovery and prevention
Can the insoles be put in any shoe?
Almost any, but not all are ideal. The insole needs a shoe with a removable last, firm counter and enough volume not to squeeze the forefoot. It does not work well in flat ballerinas, flip-flops or thin high heels. It is usual to make two insoles (one for everyday shoes, one for sports).
Is it necessary to stop running during treatment?
Generally no. In most cases we maintain the activity by reducing volume by 30-40% during the first 3-4 weeks. If there is associated acute tendinopathy, we advise stopping running for 2-3 weeks and replacing it with cycling or elliptical training. Gradual return: a prolonged total break is usually counterproductive.
Scientific references
- Barton CJ, Bonanno DR, Carr J, Neal BS, Malliaras P, Franklyn-Miller A, Menz HB. Foot and ankle characteristics in patellofemoral pain syndrome: a systematic review and meta-analysis. J Orthop Sports Phys Ther. 2010;40(11):700-14. [PMID: 20710097]
- Mills K, Blanch P, Dev P, Martin M, Vicenzino B. A randomised control trial of short term efficacy of in-shoe foot orthoses for anterior knee pain. Br J Sports Med. 2012;46(4):247-52. [PMID: 21622953]
- Hinman RS, Bennell KL. Advances in insoles and shoes for knee osteoarthritis. Curr Opin Rheumatol. 2009;21(2):164-70. [PMID: 19339927]
- Esculier JF, et al. Combining gait retraining or exercise programme with education in runners with patellofemoral pain. Br J Sports Med. 2018;52(10):659-666. [PMID: 28798040]
- Collins NJ, et al. 2018 Consensus statement on exercise therapy and physical interventions for patellofemoral pain. Br J Sports Med. 2018;52(18):1170-1178. [PMID: 29925502]
- Bonanno DR, et al. Effectiveness of foot orthoses for the prevention of lower limb overuse injuries. Br J Sports Med. 2018;52(5):298-302. [PMID: 28855184]
This page is for information purposes only and does not replace the individual clinical assessment. Each case requires a personalized examination.
Don’t let knee pain control your day-to-day life
If you’ve been convinced for months that your knee is “just the way it is”, give the biomechanical study a try. Sometimes the answer has been on the floor for years.
- 📞 +34 965 921 156
- ✉️ info@clinicasanroman.com
- Av. del Dr. Ramón y Cajal 1, 03001 Alicante