
PERCUTANEOUS SURGERY FOR CLAW TOES AND HAMMER TOES
Surgery for Claw Toes and Hammer Toes in Alicante
Straight toes, no painful calluses, no screws, and walking home.
If you’ve been dealing with bunions, calluses, and pain every time you walk or try on closed-toe shoes for years, this page is for you. At Clínica San Román, we have been correcting minor toe deformities for over 45 years, and today we perform minimally invasive percutaneous surgery (MIS): millimeter-long incisions, local anesthesia, and most patients walk out on their own the same day.
⭐ 4.8/5 (190 Google reviews) · 🏅 Cert. MIS23BE03 (American Board) · 🇪🇺 Service available in 5 languages

Backed by 45 years of experience
45+ years old
Family clinic founded in 1979
🏅 MIS23BE03
First in Europe to receive American Board certification in minimally invasive foot surgery
⭐ 4.8
190 verified reviews on Google
🇪🇺 5
Languages: ES · EN · NL · FR · DE
Led by Dr. José Manuel San Román Pérez (founder) and Dr. Israel San Román Sirvent, a Fellow of the American Academy of Ambulatory Foot & Ankle Surgery since 1986.

What are claw toes and hammer toes?
Both are progressive deformities of the smaller toes (the 2nd through 5th toes) in which the joints are permanently bent. They can affect a single toe or several toes at once, and are the most common forefoot deformities after bunions.
The difference between them is the joint involved:
- Hammer toes: The toe bends only at the proximal interphalangeal joint. The toe resembles an “inverted V.”
- Claw toes: both interphalangeal joints (proximal and distal) are flexed. The finger is completely curled inward.
- Mal let toe: only the distal interphalangeal joint—the one closest to the toenail—bends.
Over time, the friction between the bent area and the shoe causes calluses, helomas (hard calluses), and pain when walking. The deformity starts out flexible—it can be straightened by hand—and progresses until it becomes rigid, with dislocation of the metatarsophalangeal joint.
Who does this affect?
These are common deformities: their prevalence increases with age, and they are up to five times more common in women than in men. They often occur in conjunction with hallux valgus (a bunion), because the displaced big toe pushes against the second toe, causing it to become deformed.
Symptoms: How do you know if you have a claw toe or a hammer toe?
The symptoms develop gradually. At first, it seems like just a cosmetic issue, but it eventually starts to interfere with daily life:
- A visibly bent toe that does not lie flat against the ground.
- Calluses and corns on the back of the toe (where it rubs against the shoe) and/or on the sole (under the metatarsal head).
- Pain when walking, especially in closed-toe shoes.
- Difficulty finding comfortable shoes. You avoid closed-toe shoes and heels.
- Recurrent blisters or sores on the back of the affected finger.
- Associated metatarsalgia (pain in the ball of the foot), because the toe can no longer provide support.
- Progressive stiffness: at first, the finger can be straightened, but later it can no longer be straightened.
🔴 When to seek help without delay
- The finger no longer straightens when you try to do so with your hand.
- Ulcers or open sores appear that do not heal.
- If you have diabetes and calluses are starting to form, you’re at high risk for complications.
- The pain makes it difficult for you to walk or play sports.
- You’ve tried insoles, arch supports, and switching shoes , but there’s no improvement.
The more rigid the deformity becomes, the more complex the subsequent correction is. Seeking medical advice early on makes treatment much easier.

Why do claw toes and hammer toes develop?
There is rarely a single cause. The deformity occurs when the intrinsic muscles of the foot (flexors and extensors) lose their balance:
- Foot type and biomechanics — cavus foot, short first toe (Morton’s toe), ligamentous hyperlaxity.
- Associated hallux valgus (bunion) — the misaligned big toe pushes against the second toe, causing it to become deformed.
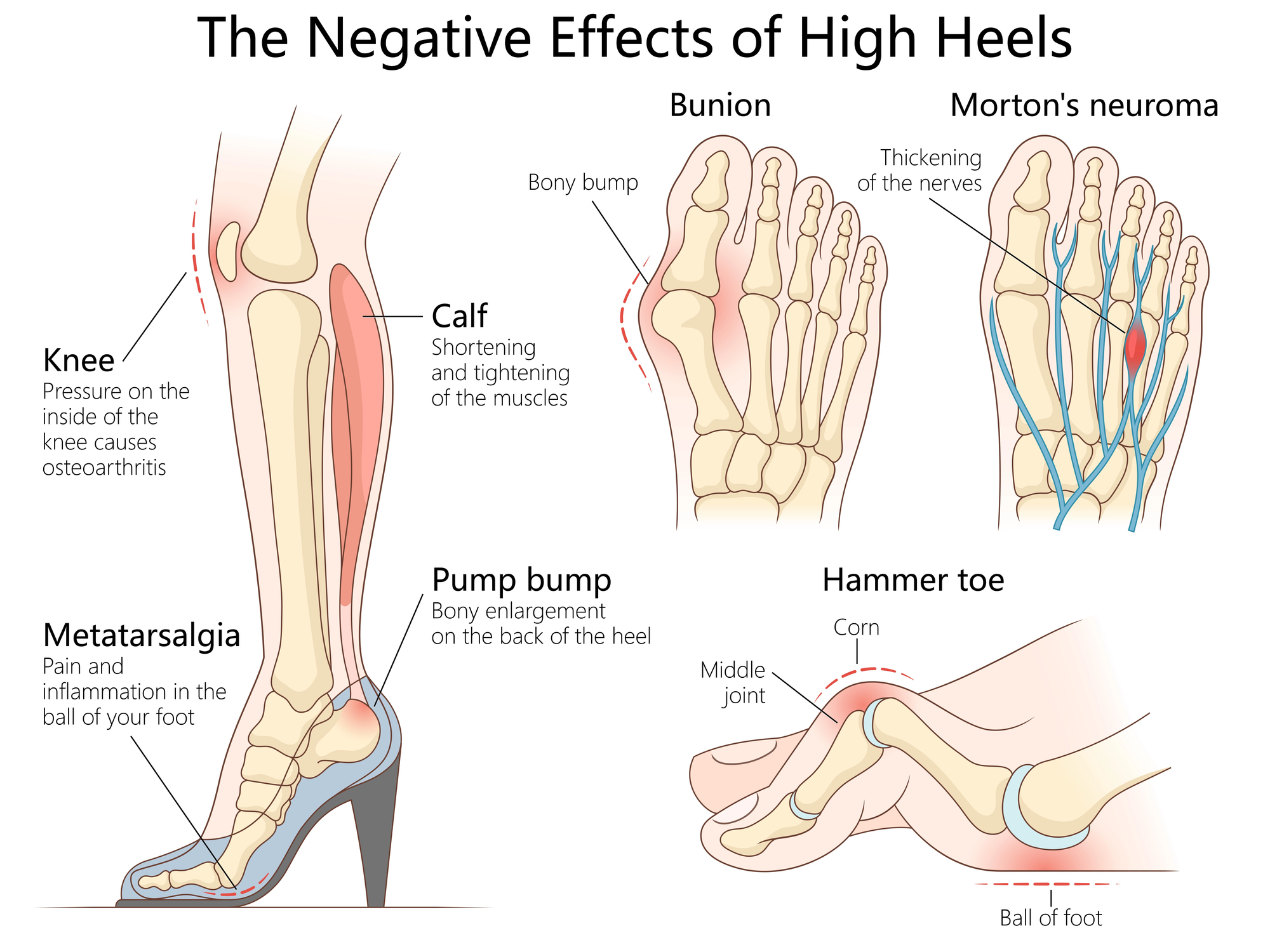
- Inappropriate footwear —high heels and narrow toes—for years force the toes into an unnatural position.
- Rheumatic diseases — rheumatoid arthritis, psoriatic arthritis, gout.
- Neuromuscular disorders — Charcot-Marie-Tooth disease, post-stroke sequelae, diabetic polyneuropathy.
- Previous injuries — finger fractures, repeated sprains, tears of the plantar fascia.
- Age — tissues lose their elasticity, and the deformity progresses over time.
In many cases, several factors are at play. That is why treatment must address the underlying cause of your finger condition, not just correct its appearance.
Can claw toes be corrected without surgery?
It depends on the severity of the deformity. As long as the finger remains flexible, conservative treatments can provide significant relief from symptoms for years:
- Wide-fitting shoes with a high toe box (doesn’t squeeze the top of the toe).
- Custom insoles that relieve pressure on the metatarsal heads and alleviate associated metatarsalgia.
- Silicone toe separators and sleeves to protect calluses.
- Stretching and strengthening exercises for the intrinsic muscles of the foot.
- Regular foot care to manage painful calluses.
⚠️ What these measures DO NOT do: they do not straighten a finger that is already stiff, nor do they correct the bone deformity. They are merely palliative. If your finger no longer straightens on its own or the pain is affecting your daily life, minimally invasive surgery is the definitive solution.
Minimally invasive surgery for claw toes and hammer toes
Millimeter-precise incisions. Local anesthesia. Same-day discharge. No screws or fasteners required.
Correction of the smaller toes using percutaneous surgery (MIS: Minimally Invasive Surgery) has become the current European standard for treating claw toes, hammer toes, and mallet toes. Pioneers such as Redfern and Vernois (United Kingdom/France) and De Prado (Spain) have developed the third-generation MIS techniques that we use today at Clínica San Román.
Dr. Israel San Román was one of the first doctors in Europe to obtain a certification in Minimally Invasive Foot Surgery from the American Board of Multiple Specialties in Podiatry (certificate MIS23BE03). He has been a Fellow of the American Academy of Ambulatory Foot & Ankle Surgery since 1986 and is a member of GRECMIP, AMIFAS, AEMIS, and AOFAS.
What does the technique involve?
Using 2–3 mm incisions and under local anesthesia, the surgeon performs the following procedures (as needed for each finger):
- Percutaneous tenotomy of the extensor or flexor tendon to release the tension that keeps the finger bent.
- Percutaneous osteotomy of the proximal phalanx to correct structural bone deformity.
- Capsular release of the metatarsophalangeal joint in cases of dislocation or subluxation.
- Proximal interphalangeal (DIP/PIP) arthroplasty when the joint is severely degenerated.
The key: all procedures are performed under fluoroscopic guidance (real-time X-rays), without making an incision in the skin. There is no visible scar, and no internal bone fixation devices are used.

Traditional open surgery vs. MIS at Clínica San Román
| Traditional open surgery | MIS at Clínica San Román | |
|---|---|---|
| Incision | 2–3 cm per finger | Millimeter (2–3 mm) |
| Anesthesia | Regional or general | Local |
| Internal fixation | Kirschner wires, screws, or implants | Without osteosynthesis hardware |
| Income | Regular | Outpatient — same-day discharge |
| Removal of needles | Required at 4–6 weeks | Not applicable |
| Wandering | Initial immobilization | You can walk the same day in your post-operative shoes |
| Recurring sick leave | 4–8 weeks | 2–3 weeks |
| Scar | Visible on the back of the finger | Virtually imperceptible |
▶ Video: Real-world results following MIS foot surgery
Dr. Israel San Román discusses the recovery of a foot that underwent surgery using a minimally invasive technique.
Realistic recovery after MIS surgery
- Day 0: You’ll be walking in a post-operative shoe and a compression bandage. Little to no pain.
- First week: Rest as much as possible with your foot elevated. Take short walks.
- Weeks 2–3: Removal of bandages. Gradual return to sedentary work activities.
- Weeks 4–6: Wear regular-width shoes. Resume low-impact sports.
- Recurrence: rare if the underlying cause is also treated (associated hallux valgus, footwear, biomechanics).


Your first appointment at Clínica San Román
The initial consultation is free and requires no obligation. In 30 minutes, we’ll have the answer:
- Physical examination of each toe: flexible or stiff? Is there associated metatarsalgia? Is there a bunion that should be treated at the same time?
- Weight-bearing X-rays to assess the degree of deformity and examine the metatarsophalangeal joint.
- Biomechanical gait analysis when a functional cause is suspected.
- Personalized treatment plan: which toes to operate on, what techniques to use, and what to expect during recovery.
- Fixed price, no surprises.
We provide services in Spanish, English, German, French, and Dutch. We are a leading clinic on the Costa Blanca for patients from the Netherlands, Belgium, Germany, the United Kingdom, and France who travel to Alicante for surgery.
Frequently Asked Questions About Claw Toes and MIS Surgery
📋 About your case
🏥 About the surgery
❌ Myths to Debunk

Straight toes, no calluses, and no pain when walking
If you’ve been dealing with bunions, recurring calluses, and shoes that no longer fit for years, now is the time to take action. The initial consultation is free and requires no obligation. In 30 minutes, we’ll clear up any doubts: whether your fingers are suitable for MIS surgery, what your recovery will be like, and what results you can expect.
📞 +34 965 921 156
✉️ info@clinicasanroman.com
📍 Av. del Dr. Ramón y Cajal 1, 03001 Alicante
🌐 Service available in Spanish, English, German, French, and Dutch